 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
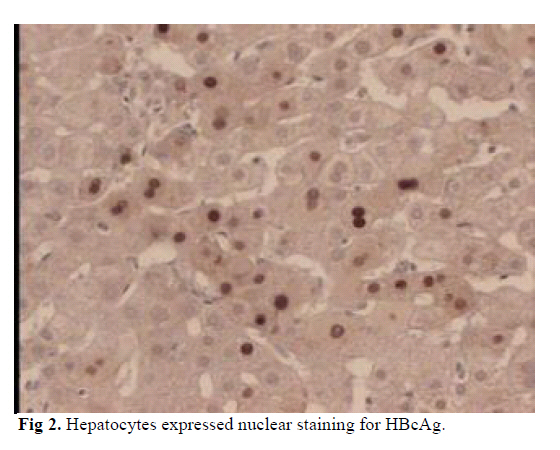
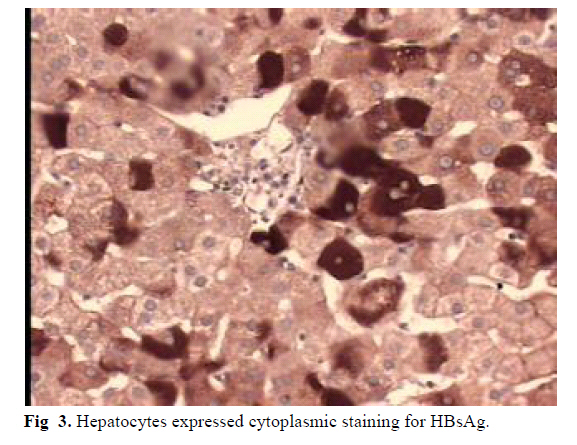
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 2, July, 2006, pp. 98-100 CASE REPORT HEPATITIS B VIRUS INFECTION IN AN ANTI-HBC NEGATIVE PATIENT: A CASE REPORT SEDIGHEH AMINI KAFI-ABAD, MD*, AND ALI TALEBIAN, MD** From the Research Center of the Iranian Blood Transfusion Organization, Tehran, Iran. Code Number: mr06022 ABSTRACTOne of the best reliable markers of hepatitis B virus infection is antibodies to the core antigen (Anti-HBc). A first-time blood donor with HBsAg positivity was identified as an HBV carrier that was anti-HBc negative. The patient was followed for 24 months in order to investigate the evolution of his HBV serological profiles and HBV-DNA (PCR). In the follow-up for 24 months, HBsAg, HBeAg and HBV-DNA (PCR) were positive but all the time anti-HBc remained negative. HBV DNA viral load was 3.4×106 copies per mL. In the immunohistochemical study on the needle liver biopsy, the hepatocytes were positive for HBcAg and HBsAg. For this immunological situation, the most probable hypothesis is an immunotolerance to HBV due to an in utero HBV infection. This situation does not impose a risk of HBV transmission by blood transfusion, because HBsAg positive donations are excluded and discarded by HBsAg screening tests. Keywords: Anti-HBc, Hepatitis B Virus (HBV), Tolerance, Immunity. INTRODUCTION Hepatitis B virus produces several protein antigens such as HBsAg and HBeAg. HBcAg is produced by hepatitis B virus and is detected in liver tissue.1-2 Antibodies to each of these antigens can be measured in blood.1-4 3-4 weeks after the appearance of HBsAg, anti- HBc can be detected and persists for many years.5-8 In the Iranian Blood Transfusion Organization a sample from each donation is tested for HBsAg, Anti-HIV, anti- HCV and a serologic test for syphilis like RPR. All positive donation units are excluded and discarded. The positive results are confirmed, then donors are notified and they are followed-up by the Iranian Blood Transfusion Organization hepatitis clinic. CASE REPORT The first-time blood donor was a man. He was 30 years old, born and living in Tehran. At his first donation on June 2001 he was positive for HBsAg and negative for anti- HIV, anti-HCV and RPR so this unit was discarded. Four blood samples were obtained during nearly 24 months. The results obtained from the HBV serological markers included HBsAg, anti-HBc, HBeAg, HBeAb that are shown in detail in Table I. The results remained stable through-out the follow-up. HBV DNA was analyzed using polymerase chain reaction (PCR). HBV DNA was positive by PCR method and detected by gel electrophoresis (Fig 1). The HBV DNA viral load was 3.4×106 copies per ml. The needle liver biopsy on August 2001 was studied, and no significant pathologic changes were observed. The histological activity index, according to modified HIA score was A: 0, B: 0, C: 1, D: 0, Total=1 and stage: 0.9 Immunohistochemical studies were performed using HBcAg and HBsAg markers and detected by avidin-biotinperoxides complex method. The needle liver biopsy demonstrated strong nuclear reactivity for HBcAg and cytoplasmic positivity for HBsAg10, 11 (Fig 2 and 3). In order to evaluate the status of the immune system especially an efficient antiviral cellular and humoral immune response, several serological markers were studied. The results of immunoglobulin G, A and M were in references interval according to age and sex. The patient exhibited antibodies to cytomegalovirus (6.8 IU/mL, Reference Value: Immunity>1.1 Iu/ml). The patient's mother was evaluated for HBV infection and she was positive for HBcAb. DISCUSSIONAnti-HBc negativity in HBsAg positive carrier children and blood donors has been reported in a few studies.12-14 In one study in China the absence of anti-HBc occurred in four children who were infected perinatally. They were HBsAg and HBV DNA positive but anti-HBc never appeared.13 Two blood donors in France exhibited such a profile.14 Hepatitis B infection and failure to produce anti-HBc after several months has been described in three different circumstances. First, unresponsiveness to viral infection and antigens like HBV infection and HBcAg are encountered in immunocompromised patients.15,16 Second, some partial deletions in the core gene have been detected in HBV infection. These deletions cause the reduction of HBsAg, HBcAg and HBeAg and their antibodies or absence of anti-HBc and other antibodies.17,18 Third, anti-HBc has been found to be negative in some infants who were HBsAg positive and were borne to HBeAg positive carrier mothers.14,19-23 It is suggested that HBeAg can cross the placenta and establish T helper cell tolerance in utero for HBeAg and HBcAg.14,22 These results support immune incompetency of the hepatitis B virus antigens in neonates, so HBsAg carrier infants with serum anti-HBc negativity may result from immunologic tolerance in the uterus. In this case the first hypothesis was excluded because the patient did not have hypogammaglobulinemia and produced antibodies against other viruses like CMV. HBsAg and HBcAg were produced and detected in liver tissue and in long-term follow-up HBV antigens were detected in blood (Table I), so the second hypothesis was unlikely. The third hypothesis seems to be the probable explanation for this immunologic and clinical situation. Serological markers and results of HBV DNA viral load indicated active viral replication but no significant pathologic changes were observed in liver biopsy. These findings were in agreement with possibility with an immune incompetence to HBV infection in this subject. Long term follow-up of the patient in the future was recommended because a delayed immune response could not be definitively excluded. This situation does not impose a risk of HBV transmission by blood transfusion because HBsAg positive donations are excluded and discarded by an HBsAg screening test. REFRENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06022f2.jpg] [mr06022f3.jpg] [mr06022f1.jpg] [mr06022t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}