 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
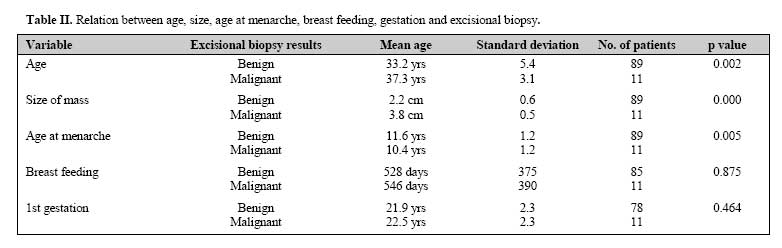
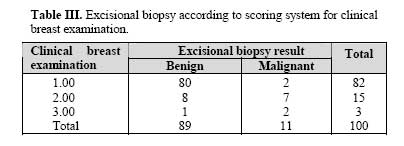
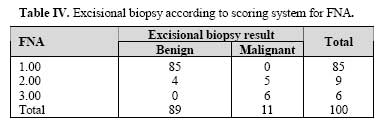
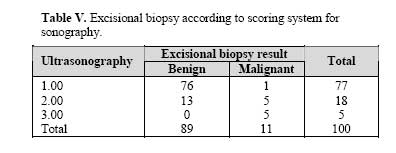
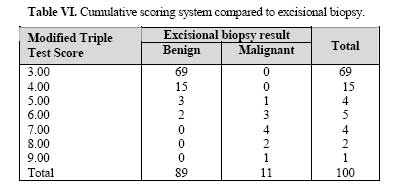
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 3, November, 2006, pp. 115-118 Modified Triple Test Score (MTTS) for Evaluation of Palpable Breast Masses in Women Under Age 40 A. Ghafouri, M.D.,* SH. Attarian, M.D.,† M. Tavangar, M.D.,† and N. Sedighi§ From the Dept of Surgery, Dr Shariati Hospital, Tehran University of Medical Sciences, Tehran, I.R. Iran. Code Number: mr06026 ABSTRACT Background: Evaluation of breast masses in women under 40 years old starts with a Triple Test Score (TTS) which is composed of clinical breast examination, mammography and fine needle aspiration. Increased breast density in this age group decreases the sensitivity of mammography. So deciding whether to biopsy such nondiagnostic lesions or not is subject to challenge. Breast masses up to 2mm could be observed by ultrasonography using probes with high frequencies (10-13 MHz) with a specificity and sensitivity of more than 80%. Keywords: Breast mass, FNA, Sonography, Mammography INTRODUCTION Breast masses in young women are common. Each year thousands of women present to general surgeons with palpable breast masses, some of which are clinically ambiguous and the majority of which are benign. Although the probability of cancer may be exceedingly small, it is never zero. So careful evaluation, exact diagnosis and definite treatment are mandatory in any breast mass.1-4 The dilemma that the dogmatic statement “every palpable mass in the breast must be excised" should be replaced by the recommendation" every palpable mass must be assessed and clarified".5 Evaluation of a palpable breast mass starts with components of the triple test including clinical breast examination, mammography and fine needle aspiration alone or in combination, While open biopsy provides more data, it results in undesirable cosmetic problems.2, 4, 6, 7 There is strong evidence for the value of using the triple assessment to estimate the probability of malignancy and guide the evaluation of palpable breast mass. Each component of the triple test assigns score number 1 when it appears benign, number 2 when it appears suspicious and number 3 when it appears malignant and the sum of scores is called the triple test score (TTS).When the triple assessment is performed adequately and produces concordant results (all benign or all malignant) or scores are above 6 (malignant) or under 4 (benign) the diagnostic accuracy approaches 100%. However 40% of cases are nonconcordant and masses with score 5 require open biopsy.4, 5, 8-15 When the components of the triplet all point to benignity, the patient may be confidently followed up without the necessity of biopsy and adoption of these guidelines may safely reduce the number of open breast biopsies by about 50-60%.16 Due to the reduced sensitivity and specificity of lesion detection by mammography in young women under 40 and the usefulness of sonography in this group of patients, researchers dealing with women under 40 combined sonography with mammography to the scoring system and the modified triple test score (MTTS) was introduced which is an integration of clinical breast examination, sonography and FNA.24, 25 Since the study in this field is limited this study was designed to explore the role of MTTS on evaluation of breast masses in women under 40 years old. PATIENTS AND METHODS An observational study was designed to evaluate as many as 100 cases of women with palpable breast mass under 40 who had referred to Tehran Shariati Hospital, Tehran Institute of Cancer (Meraage) and Milad Hospital during a period of 19 months (from March of 2003 to October of 2004). All cases were examined by a general surgeon and afterwards referred to a sonographist for bilateral breast sonography. Fine needle aspiration of breast mass was done by means of a number 21 gauge needle attached to 5 mL syringe. Six smears were prepared, dried in free air and then fixed with % 96 ethylic alcohol and sent for cytology. As a gold standard, excisional biopsy was done to compare results. Recommended scores for benign, suspicious, and malignant findings in clinical breast examination, sonography and FNA were 1, 2 and 3 respectively. Modified Triple Test Score (MTTS) as the sum of these scores were compared with excisional biopsy results at last. SPSS Version 11.5 performed analysis of data. RESULTS Mean age of the study population was 33.6 ± 5 with a range of 20 to 40 yr. Mean dimension of breast mass-measured by sonography was 2.4± 0.8 cm (1-5 cm). Age of first gestation was reported between 16 to 26 years of age with a mean of 22±2.3 yr. Age of first menstruation was between 9 to14 years old with a mean of 11.5± 1.3 years old. Total breast feeding time period was 48 months at maximum with a mean of 528 days in general. Comparison of these variables in malignant and benign groups is reported in Table II. Results of excisional biopsy according to scoring system for clinical breast examination, sonography and FNA are shown in Table III, IV and V. MTTS as the cumulative scoring system may be compared with excisional biopsy results as shown in Table VI. Diagnostic capability of clinical breast examination, sonography, FNA and MTTS are compared in Table VII. DISCUSSION Gobler16 in a retrospective study of 207 palpable breast masses found out that if the result of combined evaluation of clinical examination, mammography and cytological examination were concordant, a 100% diagnostic accuracy was present and with discordant results 75% of masses were malignant. He concluded that preliminary biopsy and frozen section may be unnecessary when the diagnostic triplet unequivocally demonstrates malignancy. There is strong evidence for the value of using the triple assessment to diagnose cancer in women with breast cancer. A review of 15 follow up studies showed that triple assessment is consistently more sensitive than any single test alone, capable of picking up 95% to 100% of cancers when at least one component is positive. When all three tests gave the same result, whether positive or negative, the probability that the diagnosis is correct is about 99%.17 In essence the triple test assessment is a feasible, accurate and reliable guide with diagnostic effectiveness for treatment of palpable breast masses and is equivalent and cheaper when compared to open biopsy and can be carried out in a single visit saving time. It is obviously of great importance in reducing morbidities and expenses in breast mass evaluation by preventing unnecessary surgeries.8, 11, 12, 18-21 The accuracy of triple assessment depends on the skills of those who carry out the procedures and assess the results. Crone22 in a prospective study of 200 palpable breast tumors of 200 women compared the diagnostic specificity and sensitivity of clinical examination, mammography, and fine needle aspiration alone and in combinations. In this study all tumors were excised and examined histologically, and 38 were malignant. He believes that it is statistically possible to overlook a few malignant tumors when using these three procedures. He advises that all palpable breast tumors should be excised. Donegan3 and Dennis23 believe that a solid mass in the breast requires a firm diagnosis and this usually calls for removing the lesion for histological examination. Breast mass size, lower age at menarche and old age were accompanied by greater possibility of malignancy in this study. Breast-feeding duration and age at first live birth showed no significant difference between two groups in contrast to previous studies20 possibly due to narrow age spectrum in our study. Dimensions of breast mass were of no importance in previous studies, but in our study it could be considered as a risk factor. FNA with a higher sensitivity and specificity than sonography and clinical breast examination is a better diagnostic tool. Specificity and sensitivity of the modified triple test (MTTS) in diagnosing the pathology of the mass was 100% in scores 3,4,7,8, and 9. According to the necessity of evaluation of breast mass in women under 40, MTTS can provide valuable information as follows: 1) Scores 3 and 4 could be followed up unless abnormal changes occur during this period of time. The results of this study are somehow in concordance with other larger studies published in the literature. For example, Mansoor15 in his study on 16 specimens found that all scores above 6 were malignant except one case that scored 5. He concluded scores 6 or higher are malignant and should undergo definitive therapy and masses with score 4 require open biopsy. As shown, these results are similar to our research results and are somehow repeated. CONCLUSION When scores 5 and 6 were excluded the diagnostic accuracy of MTTS was 100%. Masses scoring 4 points are benign. Seven up to nine points may proceed to definitive therapy. Five and six points need evaluation. This approach avoids open biopsy in the majority of cases while capturing all malignancies. We concluded that all scores above 6 were malignant. As observed in this study, age, size of breast mass and age at menarche may be considered as malignancy risk factors, but surprisingly in contrast to previous studies age of first gestation and total breast feeding period are not correlated. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06026t6.jpg] [mr06026t1.jpg] [mr06026t3.jpg] [mr06026t2.jpg] [mr06026t4.jpg] [mr06026t7.jpg] [mr06026t5.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}