 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
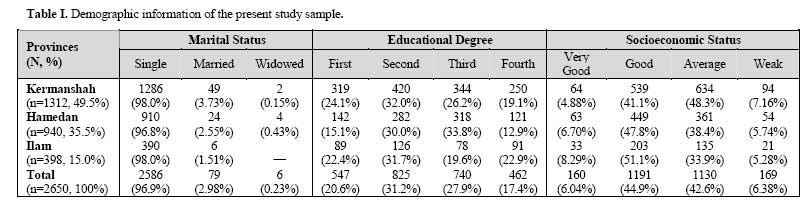
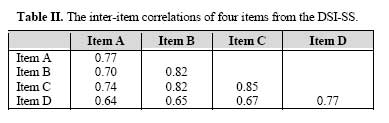
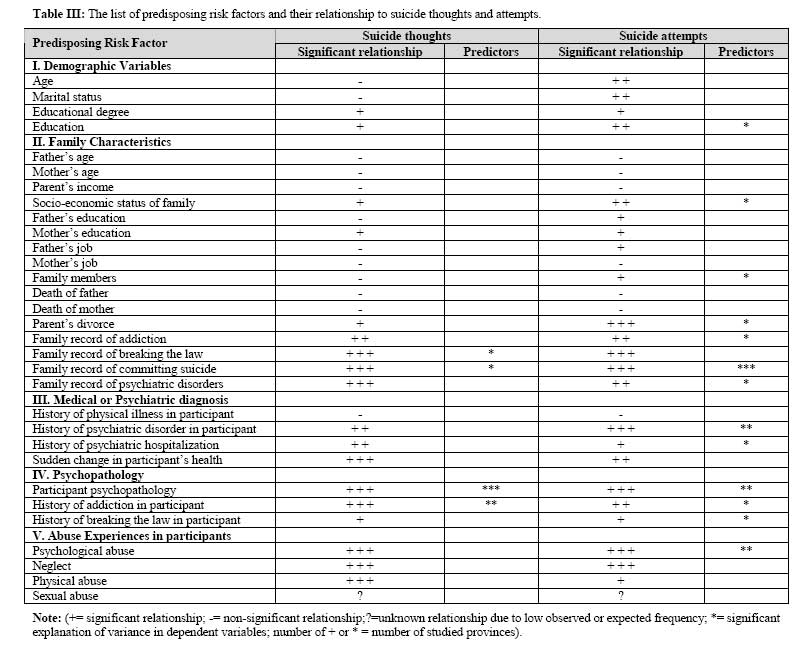
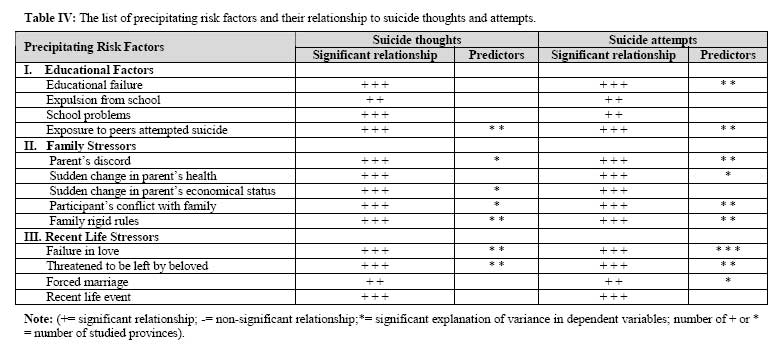
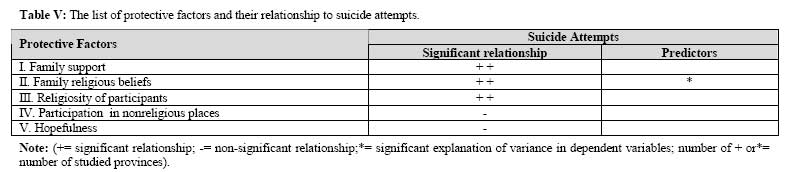
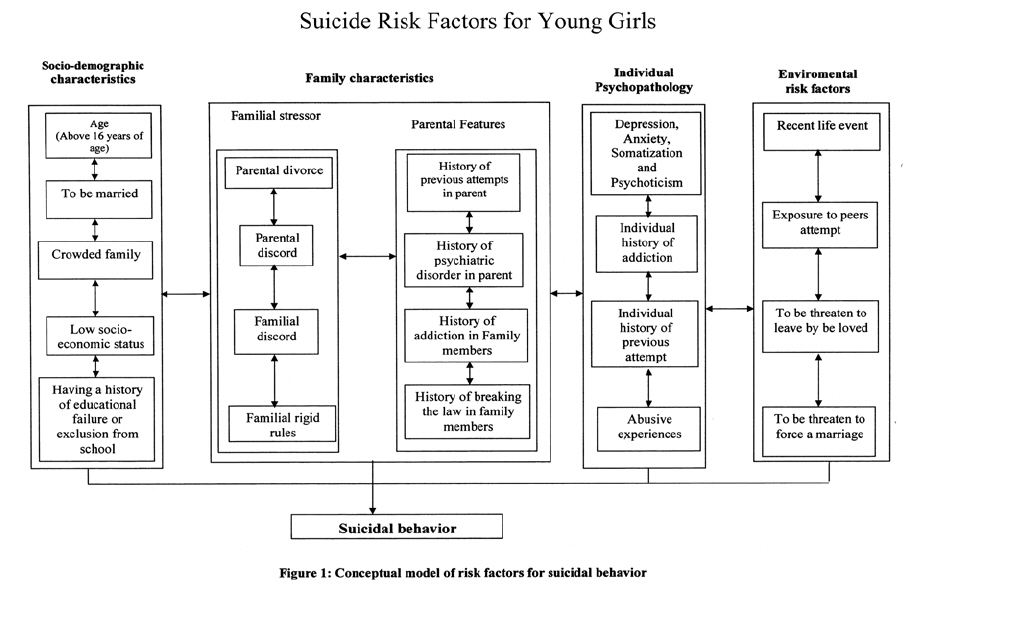
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 3, November, 2006, pp. 123-129 Predisposing and Precipitating Risk Factors for Suicide Ideations and Suicide Attempts in Young and Adolescent Girls P. Mohammadkhani, Ph.D.,* m.r. Mohammadi, M.D.,† A. Delavar,† K.S. khushabi, M.D.,§* E. Rezaei Dogaheh, M.Sc.,** and H. Azadmehr, M.Sc.†† From the University of Welfare & Rehabilitation Sciences, Tehran, Rozbeh Hospital, Tehran University of Medical Sciences, Tehran, and Allameh Tabatabaee University, Tehran, Iran. Code Number: mr06028 ABSTRACT Background: To investigate the predisposing and precipitating risk factors for suicide ideations and suicide attempts in young and adolescent females, we tried to introduce a holistic model of suicidal behavior in young and adolescent girls. Keywords: Suicide ideations, Suicide attempts, Predisposing factors, Precipitating factors INTRODUCTION In recent years, there have been growing concerns about increasing rates of suicide in adolescents. The trend has been clearly evident in some provinces of Iran with statistics reporting rising rates of youth suicide since the 1990s. Although international comparisons (National Center for Health Statistics, 2001) show that Iran has a low rate of suicide among 72 countries (0.1 per 100.000), the rate is high (29 per 100.000) in parts of the country (Center for Social Studies of Iran prime ministry, 2002). In 1998, the world rate of female suicide mortality for 15-to 24-year-olds was 7.7 per 100,000 (National Center for Health Statistics, 2001). In the United States the ratio of male to female suicide in young children was approximately 3:1, but thereafter the rate increased rapidly for boys and slightly for girls, so that among 15-to-19 yearolds it was 4.5:1 and among 20-to-24-year-olds it was greater than 6:1.1 The incidence of attempted suicide is disproportionately high among single adolescent girls.2 The concept of suicidal behavior includes thoughts about causing intentional self-injury or death (suicidal ideas) and acts that cause intentional self-injury (suicide attempt) or death (suicide). Some researchers believe that suicidal behavior involves a continuum that includes non-suicidal behavior, suicidal ideas, suicide attempts, and suicide.3 Researchers4-6 suggested that certain factors, such as depression, death preoccupation and general psychopathology are directly proportional to the severity of suicidal behavior. Suicidal behavior is a complex symptom that is markedly influenced by sociocultural factors and on a more microscopic level by presence of psychiatric disorders, other psychiatric symptoms, stressful life events, and poor social adjustment. As Lewis3 noted, “to better conceptualize the components of youth suicidal behavior, a multiaxial approach, similar to that of the DSM-IV classification for psychiatric disorders, may be utilized as a model of integrating the multifocal attributes associated with suicidal behavior in children and adolescents”. Controlled studies of suicide suggest similar risk factors for boys and girls.7 The most significant risk factor for girls is the presence of major depression, which, in some studies, increases the risk of suicide 20-fold.8 The next most important risk factor is a previous suicide attempt, which increases the risk of suicide significantly.9 In order to better conceptualize and examine the vast range of relevant variables in suicide ideation and suicide attempt, they could be outlined in accordance with three related categories: (a) predisposing or background, (b) precipitating or facilitating and (c) protecting or supporting factors. Risk factors are those conditions and events that make a person more vulnerable to the possibility of committing suicide. On the other hand, while the immediate context is critical as the precipitating cause, there are also underlying vulnerabilities which predispose certain individuals to resort to self-harming when confronted with personal crisis. These are now being designated “risk factors”. Recent works10 emphasize the need in prevention work to address both the immediate causes and the underlying risk factors. Also, such issues as unemployment and poor long-term job prospects are frequently noted as demographic risk factors of youth suicide. For example Beautrais et al.11 found that young people between the ages of 13 and 24 who had made medically serious suicide attempts were more likely to have suffered social disadvantage than other young people. In particular, they were more likely to have no formal educational qualifications. Young people who had attempted suicide are also more often found to come from disadvantaged family backgrounds, or in poor economic circumstances. There is also some evidence that young people from families with histories of parental separation or divorce have an increased risk of suicide attempt.12 The important role of family structure is also notified by many other researchers. Eshtain13 found that three out of four teenage suicides occur in households where a parent has been absent. Lester14 reported “among the possible contributing factors, only divorce rates were consistently associated with suicide and with homicide rates”. Beautrais15 reviewed a series of studies about increased rates of suicidal behavior in young people with histories of exposure to parental psychopathology including depression, substance abuse disorder and antisocial behavior. She also pointed to the importance of parent – child relationships: “there is consistent suggestion that impaired parent-child relationship, poor family communication styles, extremes of high and low parental expectations and control are associated with increased risk of suicidal behaviors among adolescents”. A further set of risk factors for youthful suicidal behavior comprises individual and personal psychopathology. Young people with mood disorders have a markedly increased risk of suicide.16 Depression is involved in over half of all attempted suicides.2 Therefore psychiatric comorbidity is a significant predisposing risk factor for suicide attempt. Kendall-Tackett, Williams and Finkebhor17 revealed the impacts of traumatic experiences, particularly sexual abuse on adolescent self-destructive and suicidal behaviors. Long-term psychological sequelae of sexual and physical abuse may include a group of psychological problems including depressive disorders, drug and alcohol abuse, suicidal behavior and somatization disorders.18 While many studies have examined risk factors for suicidal behavior, few studies have focused on the role of various social and family supports in buffering the im-pacts of exposure to known risk factors for suicide. It has been claimed that both marriage and parenthood protect against suicide.19 Rutter and Smith20 have suggested that holding attitudes and moral values against suicide may protect young people against suicide. In this study, the contribution to suicide ideation and attempted suicide of reviewed risk factors (demographic variables, family characteristics, medical or psychiatric diagnosis, psychopathology and a history of being abused) in the Iranian female population were evaluated. MATERIAL AND METHODS Participants The data reported here were collected in three stages. In the first stage, we referred to the completed suicide records of 24 provinces of Iran for the year 2002, and the provinces with the highest rates of death (Kermanshah, Hamedan, Ilam) by suicide were noted. From these three provinces 65,887 female high school students were determined as the population sampling framework for the study. In the second and third stages, through a double-stage clusteral sampling and then by simple randomized sampling, 2650 students were selected as the final sample group (their age range was 14 to 21 years; mean=16.27 years, SD=1.30 years). Table I shows the demographic features of the sample. The instrument package Data were obtained through a self-administered instrument package. The package consisted of several questionnaires that measured demographic factors and family characteristics, psychopathology, suicide thoughts and attempted suicide, hopelessness and the history of being abused. In this study, psychopathology was assessed by the Symptom Check List (SCL-90-R) inventory.21 The SCL-90-R is a 90-item self-report symptom inventory developed by Derogatis; it is designed primarily to reflect the psychological symptom patterns of psychiatric and medical patients. A preliminary version of the scale was introduced by Derogatis and his colleagues and based on early clinical experiences and psychometric analysis, was modified and validated in the present revised form.21 Each item of the “90” is rated on a 5-point scale of distress (04), ranging from “not-at-all” at one pole to “extremely” at the other. The “90” is scored and interpreted in terms of 9 primary symptom dimensions and 3 global indices of distress.21 These are labeled: I.Somatization Reliability measures concerning the 9 primary symptom dimensions of the SCL-90-R are quite satisfactory ranging between a low of 0.77 for psychoticism to a high of 0.90 for depression. About the validation of SCL-90-R, Derogatis21 indicates that “by demonstrating positive correlations between scale values and external criteria felt to be good reflection of the construct, validation is initiated”. Several studies have contrasted the SCL-90-R with other established multidimensional measures of psychopathology. Derogatis, Rickels and Rock21 contrasted the dimension scores of the “90” with scores from the MMPI. Each dimension has its highest correlation with a like construct, except in the case of O-C for which there is no directly comparable MMPI scale. Results of the study reflected a high degree of convergent validity for the “90” which represent a very important step in the validation program. Suicidality was assessed by two different sets of screening items. The first set of screening items was the suicidality subscale of the depressive symptom index.22 It is a brief screening tool for suicidality in young people in the general health setting. Table II displays the inter-item correlations of the four items from the DSI-SS suicide screen as well as corrected item-total correlations. Accordingly, coefficient alpha for the DSI-SS was quite acceptable (alpha=0.90). Also, the correlation between CES-D depressive symptoms and DSI-SS for construct validity was 0.60 (p<0.001) and correlation between DSI-SS and GHQ was 0.49 (p<0.0001).23 The second suicidality screening set of items was Lewinsohn et al's. screeners24 which were developed in the format of the CES-D. It has been used primarily in general community samples for epidemiologic/screening surveys. In a large sample of 6th to 8th grade students, responses to the Lewinsohn et al. (1996) screener were strongly correlated (r=0.70) with CES-D total scores.25 In addition, suicidal ideation as assessed with the CES-D screener was found to be related to loneliness and living in other than two-parent family. In a sample of incarcerated adolescents, several variables were found to be correlated with the Lewinsohn’s CED suicidal ideation screener (for both genders): current depression, features of borderline personality disorder, major life events, loneliness, lower self- esteem, and greater impulsivity.26 Furthermore, a brief screening measure with four questions was designed by researchers to assess the risk of suicide attempt in participants. Preliminary data on reliability for DSI-SS (α=0.89) and validity of DSI-SS and CES-D in Iranian population by calculation of their correlation with the above measure (r=0.561; p<0.001) was quite acceptable. Also, the correlation between item 59 of SCL-90-R and attempt total score (r=0.308; p<0.001) and ideation total score (r=0.504; p<0.001) was quite considerable. Child Abuse Self Report Scale (CASRS) is a 38-Item scale with four sub-scales for assessing different types of abuse. It contains (a) 14 items for psychological abuse, 11 items for neglect, 8 items for physical abuse and finally 5 items for sexual abuse.26 Procedures Because the main purpose of this study was to recognize the risk factors associated with high suicidal ideation and attempt, it was concluded that a retrospective cross-sectional design would be most feasible. To achieve the research goals, a student sample was considered most appropriate because the rates of attempted suicide were high among the population (Mohammadkhani, Rezaei Dogaheh, Nazari & Mohammadi, 2004). The data collection procedure was started by receiving permission to conduct the study from the school principals, and approval from the Research Department of the Welfare & Rehabilitation University of Iran. The administrators explained the study to students and sought their assent. On the day of data collection all students were given both written and verbal explanation of the study, and questionnaires were completed during two normal class periods. Subjects were assured of confidentiality and asked not to write their names on any part of the booklet. Given the sensitive nature of some sections of the questionnaire, an invitation was delivered to them to contact the administrator should they experience distress. Data analysis Data were analyzed using the SPSS software. (1) Based on high scores on DSI-SS, CED-SSI and researcher’s measure for assessing risk of suicide attempt, the participants were divided to “suicide ideators” and “suicide attempters” (extreme groups). Frequency and descriptive statistics were calculated to check all relevant characteristics of suicide ideators and attempters. (2) The significance of independent variables (i.e. predisposing, precipitating and protective factors)/suicide ideations and attempts, were tested with cross-tabulation analyses and t-tests. For categorical variables, Pearson’s chi-square was employed to determine any significant interaction. (3) Furthermore, we conducted multiple regression analysis for this purpose, all above factors were entered into regression for the purpose of explaining the variance in each of the two dependent variables (suicide ideations and suicide attempts), as criterion variables. (4) Finally, the proposal model of suicidal behavior was presented among the population, using the data on stages (2) and (3). RESULTS As Table III presents, among demographic variables, a significant relationship was found between educational degree (χ2= 8.55, p<0.36) and education of participants (χ2= 15.4, p<0.04) with suicide thoughts in one of the three provinces. So, they are considered as the first group of significant predisposing risk factors for suicide thoughts. Similarly, among family characteristics, socioeconomic status of the participant’s family (χ2=22.40, p<0.0001), participant’s mother’s educational level (χ2=6.679, p<0.035), parent’s divorce (χ2=5.198, p<0.023), family record of addiction (χ2=11.683, p<0.001), family record of breaking the law (χ2=4.457, p<0.035), family record of committing suicide (χ2=52.091, p<0.000) and family record of psychiatric disorders (χ2=16.925, p<0.000) had significant relationships with suicide thoughts. Comparisons revealed significant relationships between having a history of psychiatric disorder in participants (χ2=5.004, p< 0.025), history of psychiatric hospitalization (χ2=18.539, p<0.000), and sudden change in participant’s health (χ2=29.391, p<0.000) and having suicide thoughts. Participants’ psychopathology (χ2=121.112, p<0.000), their history of addiction (χ2=12.616, p<0.000) and breaking the law (χ2=0.187, p<0.665) were also significantly related to suicide thoughts. Psychological abuse (χ2=78.682, p<0.000), neglect (χ2=76.507, p<0.000) and physical abuse (χ2=15.236, p<0.000) as predisposing risk factors have strong relationship with suicide thoughts. As represented in Table IV, all subgroups of precipitating risk factors were significantly related to suicide thoughts. Educational failure (χ2= 8.43, p<0.004), expulsion from school (χ2=9.32, p<0.002), school problems (χ2=14.63, p<0.001), and exposure to peers attempt (χ2=16.17, p<0.001) had strong relationship with suicide thoughts. Among family stressors, parent’s discord (χ2=64.74, p<0.001), sudden change in parent’s health (χ2=23.73, p<0.001), sudden change in parent’s economical status (χ2=11.97, p<0.001), participant’s conflict with her family (χ2=52.26, p<0.001) and family's rigid rules (χ2=35.51, p<0.001) were significantly related to high suicide ideations. Failure in love (χ2=62.62, p<0.001), threaten to be left by beloved (χ2=100.5, p<0.001), forced marriage (χ2=13.03, p<0.001) and recent life event (χ2=41.26, p<0.001) were other precipitating risk factors, that were related to suicide thoughts. Owing to limitations of space, we dispense with presenting the results of the relationships between above risk factors and suicide attempts (see Table III, Table IV and Table V). These results can be obtained from the authors upon request. The second major type of analysis focused on multiple regression analyses. The results indicated that family record of breaking the law (χ2=126.79, p<0.0001), family record of committing suicide (χ2=126.79, p<0.0001), participant’s psychopathology (χ2=126.79, p<0.0001) and her history of addiction (χ2=126.79, p<0.000) as predisposing risk factors could significantly anticipate the suicide ideations. Furthermore, the results revealed that among precipitating risks, exposure to peers’ attempted suicide (χ2= 114.31, p<0.0001), parents’ discord (χ2=1119.82, p<0.0001), sudden change in parent’s economical status (χ2= 114.31, p<0.0001), participant’s conflict with her family (χ2=1119.82, p<0.0001), family's rigid rules (χ2=1119.82, p<0.0001) and threat to be left by beloved (χ2=1119.82, p<0.0001) anticipate the suicide thoughts, significantly. As Table IV presents, family religious beliefs were the only protective factor that could significantly anticipate the suicide attempts (χ2=12.41, p<0.02). CONCLUSION The results of the current study suggest that suicidal behavior in young females seems to happen frequently, although not invariably, in the presence of multiple risk factors which as Beautrais15 has noted “encourage the development of suicidal behaviors”. The risk factor domains that may contribute to this process include (1) sociodemographic features, (2) familial characteristics, (3) individual psychopathology, and (4) environmental risk factors. One might have to consider the influence of above risk factors that may be modified or changed by cultural and contextual features of the society and some protective factors that may act to discourage the development of suicidal behaviors. One way of summarizing these findings are suggested by the conceptual model in Fig. 1. This model assumes that there are a series of correlated sets of factors (individual, family and environmental factors) which act as effective determinants for suicidal behaviors. Risk is increased by a variety of psychological symptoms (including depression, anxiety, somatization and pychoticism), having a history of addiction and traumatic experiences particularly previous attempts. As Shaffer8 indicated “stressful events occur commonly within most adolescent suicides”. So, recent stressful life events like being threatened to be left by a beloved one, forced marriage and, exposure to suicide attempts are all important environmental risk factors. Also, this model emphasizes on the role of family characteristics in attempting suicide. Disturbed and discarded parents with history of psychiatric disorders, addiction, previous suicide attempts and low socio-economic status encourage attempting suicide in family members. Finally, the likelihood that a young female will proceed to attempt or commit suicide will vary as a function of cultural milieu and power of the protective factors. ACKNOWLEDGEMENTS The authors are especially grateful to the Women's Branch of the Prime Minister Foundation for its financial support. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06028t2.jpg] [mr06028f1.jpg] [mr06028t3.jpg] [mr06028t4.jpg] [mr06028t1.jpg] [mr06028t5.jpg] [mr06028f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}