 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
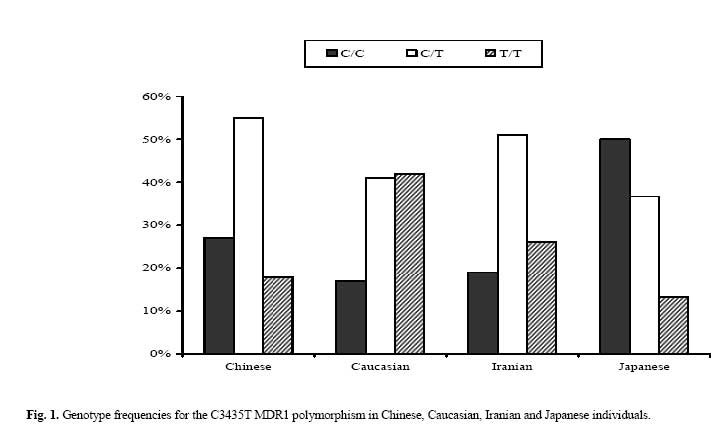
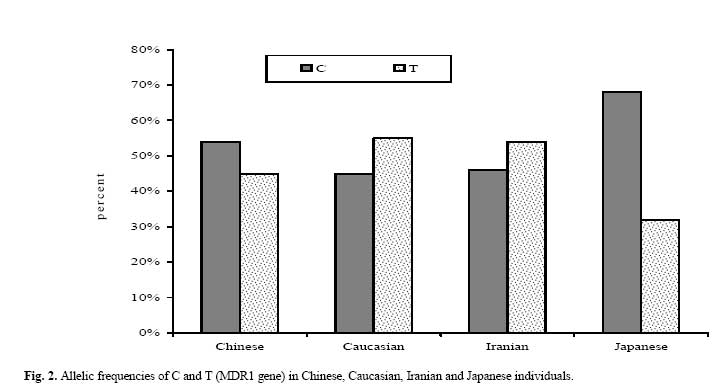
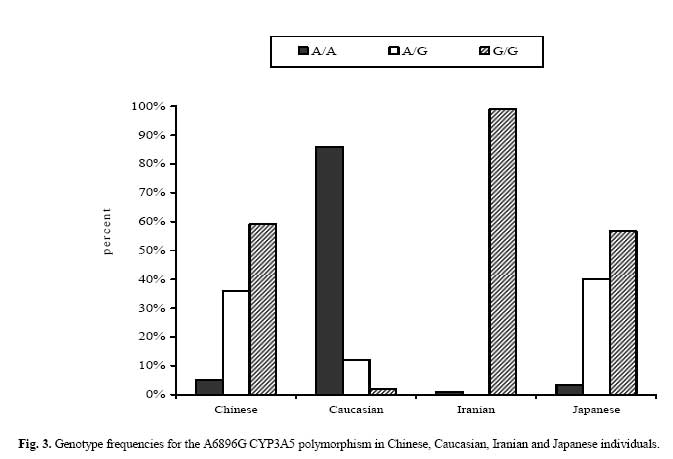
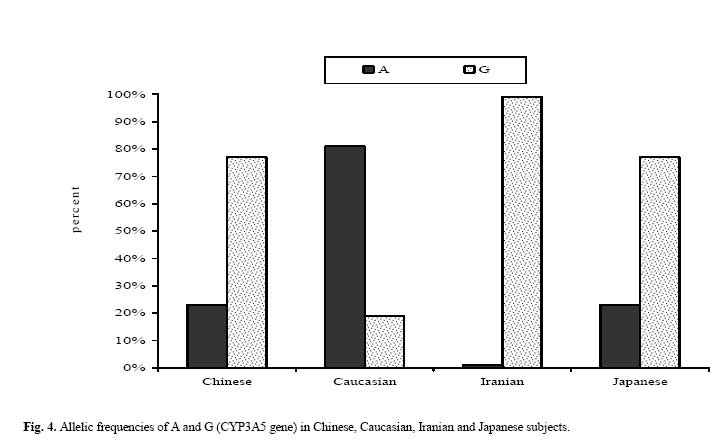
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 3, November, 2006, pp. 131-136 Frequency of C3435 MDR1 and A6896G CYP3A5 Single Nucleotide Polymorphism in an Iranian Population and Comparison with Other Ethnic Groups N. Azarpira, M.D.,* and M.H. Aghdaie, M.Sc.† From the Organ Transplant Research Center, Shiraz University of Medical Sciences, Shiraz, Iran. Code Number: mr06029 ABSTRACT Background: It is well recognized that different patients respond in different ways to medications. The inter-individual variations are greater than the intera-individual variations, a finding consistent with the notion that inheritance is a determinant of drug responses. The recent identification of genetic polymorphisms in drug-metabolizing enzymes and drug transporters led to the hypothesis that genetic factors may be implicated in this interindividual variation. Single nucleotide polymorphism in common metabolic pathway, cytochrome P450 and common transporter, multidrug resistance-1 gene are two important sites that might involve clinically significant genetic variations. Ethnicity greatly influences these genetic polymorphism distributions. Keywords: MDR1, CYP3A5, Polymorphism, Iranian population INTRODUCTION Genetic polymorphisms are implicated in the interindividual variability of the pharmacokinetic and pharmacodynamic characteristics of many drugs. Interindividual variations are greater than the intraindividual variations, a finding consistent with the notion that inheritance is a determinant of drug responses. In the general population it is estimated that genetics accounts for 20% to 95% of the variability in drug disposition and effects.1, 2 Many other nongenetic factors, such as organ function, drug interactions, and the nature of the disease, probably influences the effects of medication. In the common metabolic pathway, cytochrome P450, four CYP3A isoenzymes have been identified: CYP3A4, CYP3A5, CYP3A7 and CYP3A43, among which, CYP3A4 and CYP3A5 are the major components.3, 4 CYP3A5 is expressed heterogeneously among the population and accounts for a great part of total CYP3A enzyme content in the intestine and liver. A frequent single nucleotide polymorphism (SNP) 6896A>G has been found to be associated with CYP3A5 protein production and enzyme activity.3, 4, 5, 6 The G>A mutation in intron 3 results in a splice defect of the mRNA and produces an unstable and nonfunctional protein. The mutated allele was named CYP3A5*3 and the wild type was assigned CYP3A5*1. Only individuals carrying at least one CYP3A5*1 allele can express high levels of the CYP3A5 enzyme. P-glycoprotein (P-gp), the product of the multidrug resistance gene (MDR1, called ABCB1)7,8 acts as a transmembrane efflux pump involved in energy-dependent export of xenobiotics from inside to outside the plasma membrane. It is present in intestinal epithelial cells, biliary canalicular cells, the blood-brain barrier, and the lymphocytes and on the luminal surface of proximal tubule kidney cells.9 P-gp may, therefore, affect the absorption of drugs from the gut, their distribution in the body, and their excretion.10 Several SNPs have been described in the MDR1 gene, and one of them has been shown to be associated with lower intestinal P-gp expression and activity in vivo.8-10 This SNP is a C to T exchange at nucleotide 3435 located in exon 26, which does not affect the amino acid sequence of P-gp. Individuals homozygous for the mutation at position 3435 (TT) had significantly lower P-gp levels in the small intestine compared with the remainder of the population and showed the highest plasma concentrations of some drugs after oral administration.8-10 It has been demonstrated that there is a link between the polymorphisms of cytochrome P450 and multidrug resistance-1 (MDR1) genes, and the daily dose necessary to achieve adequate blood concentrations of many drugs such as tacrolimus, an immunosuppressive drug.11 In this study, we investigate the frequency of the SNP of A6896G in intron 3 of CYP3A5 gene and C3435T in exon 26 of the MDR1 gene in the Iranian population and evaluated the CYP3A5 and MDR1 genotypes and allele frequency in 4 different ethnic groups: Iranian, Caucasian (United Kingdom), Chinese and Japanese.11, 12, 13 PATIENTS AND METHODS Two-hundred healthy unrelated Iranian subjects participated in the present study. The average age was 38.82 ± 13.16 years (range, 18-65 years). All subjects gave written consent prior to study accrual and the protocol was approved by the ethics committee of Shiraz University of Medical Sciences. DNA was extracted from a peripheral blood sample using a blood extraction kit (Fermatas, Germany) and was stored at -20°C until analysis. A polymerase chain reaction (PCR)-restriction fragment length polymorphism (RFLP) was also used for the detection of C3435T SNP. Primers were designed according to Ameyaw et al's method.10 The primers used were as follows: MDR1 F (5'-TGC TGG TCC TGA AGT TGA TCT GTG AAC-3') and MDR1 R (5'-ACA TTA GGC AGT GAC TCG ATG AAG GCA-3') A PCR assay using 0.28 μm of each primer was performed with buffer containing 10 μm Tris and 50 μm KCl, 1.5 μm MgCl2, 200 μm each of dNTP and 1 U Taq DNA polymerase. PCR amplification conditions were 8 min of initial denaturation at 94°C, followed by 35 cycles of melting at 94°C for 30 sec, annealing at 68°C for 30 sec, and elongation at 72°C for 30 sec, followed by a final extension for 10 min at 72°C. This was followed by digestion of a 248 bp PCR product with restriction enzyme Mbo I (Roche, Germany) for 2 h at 37 °C. Digested products were separated on a 2.0% agarose gel. Mbo I digestion of wild-type DNA yields fragments of 172 bp, 60 bp and 16 bp. The C3435T mutation destroys one restriction site and Mbo I digestion yields a 238 bp and 16 bp fragments to genotype the A6986G polymorphism in the CYP3A5 gene, the PCR- RFLP method was used according to Tsuchiya et al.1 The primers used were as follows: CYP 3A5 F, 5'-ATGGAGAGTGGCATAGGAGATA-3'; and CYP3A5 R, 5'-TGTGGTCCAAACAGGGAAGAAATA-3'. Briefly, PCR was performed with 50 ng of genomic DNA, 50 pmol of each primer, 100 μM of each deoxynucleotide triphosphate, 0.6 units of Taq DNA polymerase, 1.2 mM MgCl2, and 1× reaction buffer (Fermentas, Germany). PCR amplification conditions were 8 min of initial denaturation at 94°C, followed by 40 cycles of melting at 94°C for 30 sec, annealing at 55°C for 30 sec, and elongation at 72°C for 30 sec, followed by a final elongation for 10 min at 72°C. The PCR products were digested at 37°C overnight with 10 units of SspI (Roche, Germany). Digested products were separated on 2.5% agarose gel containing ethidium bromide. If the A allele (CYP3A5 *1 allele) was present, the 130 bp PCR fragment was divided into 107 bp and 23 bp fragments. Few PCR products were sequenced with a Genetic Analyzer (Applied Biosystems). Statistical Analysis The allelic frequencies were calculated based on the observed number of two different alleles, derived from genotypes data in this group. These results were compared between the Iranian population studied here and the published data of Chinese, Japanese and Caucasians (United Kingdom).11, 12, 13 The R×C contingency table analysis was used to compare the inter-ethnic differences in the distribution of alleles and genotypes, and chi- squared test was used for comparisons of two different ethnic groups. Analyses were performed with SPSS software (Statistical Package for the Social Sciences, Version 10.0, SSPS Inc, Chicago, Ill, USA), and results were considered to be significantly different when p<0.05. RESULTS The distribution of MDR and CYP3A5 genotypes and alleles among Iranian, Chinese, Caucasian (United Kingdom) and Japanese populations are shown in Table I and Table II. The three potential MDR genotypes (C/C, C/T, T/T) were as follows: Chinese frequencies were 40/55/23, Caucasian frequencies were 17/41/42, Iranian frequencies were 19/51/26, and Japanese frequencies were 50/ 37/13 (Table I, Fig.1). By comparing individual groups, there are significant differences between Iranian, Chinese and Japanese subjects within genotypic (P< 0.05), (Table I,Fig.1) and allelic distribution frequencies (p=0.01) (Table II, Fig. 2). The three potential CYP3A5 genotypes (A/A, A/G, G/G) were as follows: Chinese frequencies were 5/36/59, Caucasian frequencies were 86/12/2, Iranian frequencies were 1/0/99, and Japanese frequencies were 3/40/57 (Table I, Fig.3). Iranians carried G/A allelic distribution of 99.1 percent and different from the other three groups (Fig. 4). Caucasians had an allelic distribution of 19/81 percent, Chinese 73.27 and Japanese 76.23 percent. DISCUSSION Once a drug is administered, it is absorbed and distributed to its site of action, where it interacts with targets such as receptors and enzymes, undergoes metabolism, and is then excreted. Each of these processes might involve clinically significant genetic variations. Pharmacogenetics has a potential ability to yield a powerful set of molecular diagnostic methods that will become routine tools that enable clinicians to select medications and drug doses for individual patients. So knowledge about genetic background of every individual is very important to determine his or her specific profile. We observed a pronounced ethnic difference in the alleles and genotypic distribution of MDR1 gene between Iranian population and others11, 12, 13 This study showed that the frequency distribution of the MDR allelic variants were different between Iranian, Japanese and Chinese (P<0.02) and similar between the Iranian and Caucasian population. (p=0.06, Table I) Almost 50% of Iranian and Caucasian individuals were homozygous carriers of the variant T allele compared with 32% of the Japanese and 43% of Chinese (P<0.02, Table II). There are significant differences between Iranian, Chinese and Japanese subjects within genotypes (P< 0.05, Table I) and allelic distribution frequencies (p=0.01, Table II). More than half of Iranian subjects have at least one T allele, with lower P-gp level in small intestine. As previously discussed, these patients need lower doses of some drugs.8-10 We also noted dramatic differences in the CYP3A5 alleles and genotypes distribution between Iranian subjects with other compared populations. The frequency of the homozygous GG variant was 99% in the Iranian population compared with only 1% of them being the heterozygous G/A variant. These findings are very different from other ethic populations. Caucasian and Iranian genotype distributions were also different from each other (99% G/G in Iranians and 86% AA in Caucasians). There are significant differences in the distribution of the G/G genotype between Chinese and Caucasians (P=0.00). 70% of Chinese and 99% of Iranian subjects carried the low producer GG genotype, while the proportion of Caucasians was 2% respectively. Ninetynine percent of Iranian individuals were homozygous carriers of the variant G allele compared with about 70% of the Chinese and Japanese and 19% of the Caucasian population (Table II, Fig. 4). The frequency of A allele in our population is very low. The G/G genotype has a very low level of active cytochrome P450 enzyme and the drugs that are the substrate of this enzyme must be used cautiously. It is hoped that our results will aid in understanding the ethnic diversity of the Iranian population, and offer a preliminary basis for more rational use of drugs that are substrates for CYP3A5 and MDR in this population. Future studies on the genetic profile of the other MDR and CYP subfamilies will further illustrate the distribution of different allelic variants in the Iranian population. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06029t1.jpg] [mr06029f4.jpg] [mr06029f1.jpg] [mr06029t2.jpg] [mr06029f2.jpg] [mr06029f3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}