 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
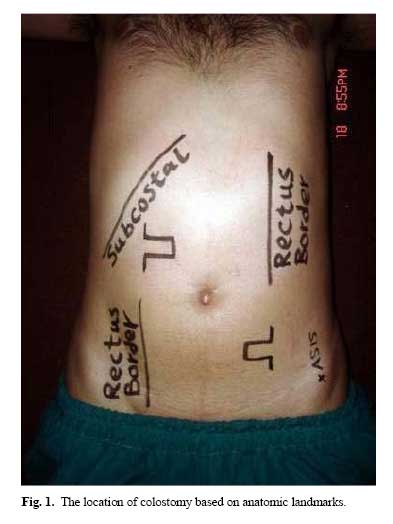
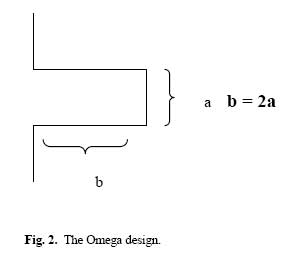
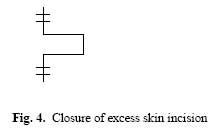
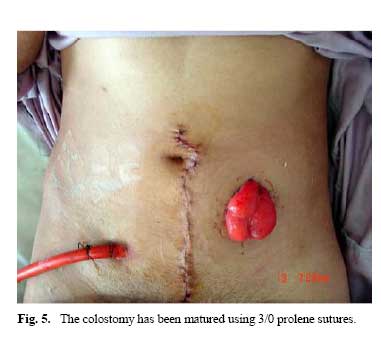
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 3, November, 2006, pp. 137-140 An Easy Solution for the Diverting Loop Colostomy: Our Technique M.R. Kalantar Motamedi, M.D., F.A.C.S,* M. Rezaei M.D.,† P. Kharazm, M.D.,* M. Sharifi, M.D.,† A. Kavyani, M.D.,† M. Zeynal Zade, M.D.,† and A.R. Saberi, M.D.‡ From the Dept. of Surgery, Shohada-e-Tajrish Medical Center, Shahid Beheshti University of Medical Sciences, Tehran. I.R. Iran. Code Number: mr06030 ABSTRACT Background: The loop colostomy is one of the most popular techniques used as a protective maneuver for a distal anastomosis and/or temporary fecal diversion. We are introducing the use of a full thickness skin bridge under the large bowel instead of a glass rod which alleviates problems such as protrusion of the large bowel, retraction of the bowel into the abdomen after removing the rod and hindering proper application of a colostomy bag over the stoma. Keywords: Penetrating rectal injury, Fournier's gangrene, Diverting loop colostomy, Skin bridge INTRODUCTION Loop colostomy is one of the most popular techniques used as a protective maneuver for distal anastomosis or for temporary fecal diversion. The current technique using a glass rod over the skin surface and underneath the large bowel prevents the retraction of the large bowel into the peritoneal cavity but doesn’t prevent further protrusion of the large bowel prevents the retraction of the large bowel into the peritoneal cavity but doesn’t prevent further protrusion of the large bowel through the created abdominal wall defect¹. It also hinders proper application of a colostomy bag over the stoma. In this article we are introducing use of a full thickness skin bridge underneath the large bowel instead of a glass rod which obviates not only the above mentioned problems of using a glass rod, but also gives a much better complete diversion similar to a double barrel colostomy without creating a double barrel colostomy. PATIENTS AND METHODS Seventeen patients needing double barrel colostomy for complete diversion of fecal material were selected using loop colostomy with skin bridge by the technique which will be discussed in detail. Three patients had Fournier’s gangrene and 14 patients had penetrating rectal injuries. This technique can be used for all patients requiring loop colostomy for any reason including protective colostomy used for low pelvic anastomosis. The reason that we did include these patients in our study was to prove the fact that it works exactly like a double barrel colostomy which is an added advantage of using this technique for creation of a loop colostomy. Operative technique An omega incision is created where we have planned for the stoma site preferably right over the rectus abdominis with the base of the bridge facing lateral as shown in Figs. 1, 2. The incision is deepened to the anterior rectus sheath creating a tongue-shaped skin bridge. The width of the skin bridge should be around 2cm and the length long enough to admit two fingers easily through the abdominal wall defect which will be created later. The extension of the incision in the shape of omega creates more space without adding to the length of the bridge unnecessarily which may increase the two by 1 ratio of the flaps and may decrease the blood supply to the end of the flap causing necrosis. The anterior rectus sheath is opened longitudinally and after splitting the rectus muscle, the posterior rectus sheath is opened transversely. These two incisions should be long enough to admit 2 fingers. In obese patients who have large epiploic appendices and thick large bowel the incision should be slightly larger not to create stenosis and difficulty in passage of fecal material. If we are using the transverse colon for loop colostomy the large bowel should be brought out through the greater omentum rather than pushing the greater omentum above the colostomy and prevent the proper coverage of small bowel by omentum. The mesenteric portion of the large bowel should be cleaned from its mesentery by ligating the vessels close to the bowel and not leaving any mesentery over the large bowel for a distance of 2cm. Then a penrose drain is passed through this hole and underneath the large bowel. The penrose drain is pulled through the stoma site which has been created as mentioned above. The large bowel in twisted 90° such that the proximal bowel stays below and the distal mucous fistula above the skin bridge which is pulled through the created hole in the mesentery of the large bowel and sutured in place as depicted in Fig. 3. If the large bowel is thin and we have excess incision more than needed, we can close part or all of the upper and lower extensions of the omega as depicted (Fig. 4). If this operation is a part of another intraabdominal operation like anterior resection we do not open the large bowel at this time and after closure of the laparotomy incision and applying a sterile dressing over the incision we only open the anterior part of the large bowel loop longitudinally over the teniae. The incision should end at least 1cm from the skin below since the large bowel may retract somewhat at the time of bowel movement through the colostomy. The colostomy bag can be put on the stoma right away. The suture used for approximating the skin bridge or closure of the extension of omega should be preferably prolene or nylon and absorbable suture should not be used (Fig. 5). RESULTS All of the 17 patients had gas passing and full passage of fecal material within 3 days post operation and they were put on oral feeding. No case of skin necrosis was encountered and no stitch abscess was observed. No parastomal hernia or large bowel prolapse was noted until the healing was completed and patients were discharged. None of the patients had any passage of fecal material through the anus until the completion of treatment period (about 10 weeks in cases of trauma and somewhat longer in cases of Fournier’s gangrene) when the patient's colostomy was closed. We didn't have any retraction of colostomy into the abdomen. For closure of the colostomy, which is best to wait at least 8 weeks to allow edema of the large bowel to subside and to have a pliable large bowel for closure, resection of the portion of the large bowel which has been used for loop colostomy is mandatory. Resection of the segment causes a better closure in the normal bowel and decreases the rate of anastomotic leak. We used bowel preparation prior to closure and we performed resection and anastomosis through the same opening (stoma site). Making an elliptical incision which is placed transversely around the colostomy, the incision is deepened down to the fascia separating the large bowel from the anterior and posterior rectus sheath to enter the free peritoneal cavity. At least 2cm of the large bowel is removed on either side of the colostomy stoma where the large bowel is pliable and not edematous. All the blood vessels leading to this segment of large bowel should be ligated close to the large bowel not causing any damage to the marginal artery of Drummond and then end to end anastomosis is performed in one layer using 3/0 silk with Gambee sutures. We did not have any anastomotic leak after closing the colostomy in the way mentioned above. The fascia of the anterior rectus is closed longitudinally and the posterior rectus sheath transversely, and skin is closed with subcutaneous absorbable suture of 2/0 or 3/0 Monocryl. DISCUSSION Fecal diversion is created in the management of patients with severe perineal soft tissue injury or in Fournier’s gangrene and also extraperitoneal anastomosis of the rectum to the large bowel. In cases where a glass rod is used underneath the loop colostomy, failure in complete diversion is usually due to colostomy retraction4, 5, 6 or prolapse.2, 3, 7, 8, 9, 10 Also it is a current belief that loop colostomy can not divert the fecal stream completely. But if the colostomy is done in the way we are suggesting complete diversion is possible. In cases for which we need to perform colostomy to decompress dilated bowel caused by a distal obstruction like in cases of obstructing rectal carcinoma, this type of colostomy can be performed without the need of another laparotomy incision. Since the skin bridge is left as long as the colostomy exists while the glass rod is removed after a while when we feel the large bowel is adequately adherent to the abdominal wall, we can never have retraction of the large bowel into the abdominal cavity with this technique. CONCLUSION Based on the results of this study we confirmed that diverting loop colostomy using a skin bridge is a safe, rapid and easy to manage colostomy technique which gives complete diversion similar to double barrel colostomy without the need of performing a laparotomy for closure of the colostomy and we recommend this tech-nique for all the cases when creation of a loop colostomy is indicated. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06030f4.jpg] [mr06030f3.jpg] [mr06030f1.jpg] [mr06030f5.jpg] [mr06030f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}