 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
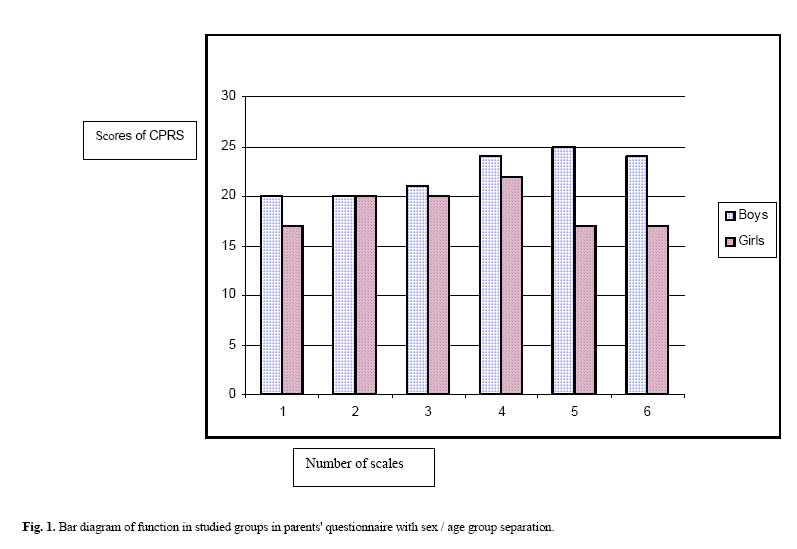
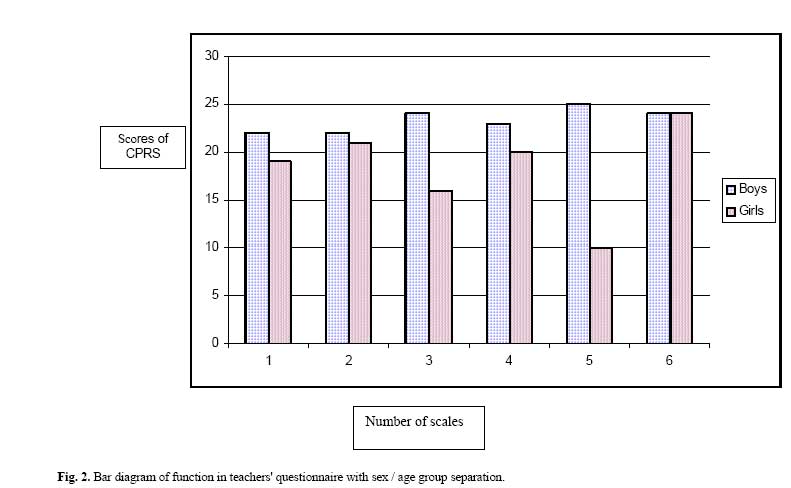
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 3, November, 2006, pp. 147-150 The Prevalence of ADHD in Primary School Students in Tehran K. Khushabi*, M.D., H. Pour-Etemad, Ph.D,† M. Mohammadi, M.D.,† and P. mohammadkhani, Ph.D.§ From the Dept. of Child Psychiatry, Dept of Psychiatry, University of Welfare and Rehabilitation Sciences, Tehran, I.R. Iran. Code Number: mr06032 ABSTRACT Background: Attention Deficit Hyperactivity Disorder (ADHD) is characterized by a developmental disorder involving inappropriate poor attention span or age-inappropriate features of hyperactivity and impulsivity and/or both. INTRODUCTION Attention Deficit Hyperactivity Disorder (ADHD) is characterized by a developmental disorder involving inappropriate poor attention span or age-inappropriate features of hyperactivity and impulsivity or both. To meet the diagnostic criteria, the disorder must be diagnosed for at least six months, cause impairment in academic or social functioning and occur before the age of 7yr.1, 2, 3 According to the fourth Diagnostic and Statistical Manual Textual Revision (DSM-IV- TR) of mental disorders, there are three subtypes of ADHD: Predominantly inattentive type, predominantly hyperactive inattentivetype and combined type.1, 2 Some impairments from the symptoms are seen in two or more settings (at school and at home).2 Most children with ADHD are between the ages of 6 to 12 yr., therefore, symptoms of the disorder are described mainly for this age group. However, it should be noted that ADHD can be problematic in the preschool age group and continue into adolescence. Also adulthood and boys have a greater incidence than girls, with the ratio being 3 to 1. The disorder is mostly common in the first born boys.1, 2 It has been estimated that more than 50% of children with ADHD are prone to experience other psychiatric disorders such as Oppositional Defiant Disorder (ODD), depression and anxiety disorder.1, 2, 4, 5 ADHD is believed to be the most common psychiatric disorder in children, affecting 3% to 5% of the school age population. It is also a condition which has been documented in many parts of the world, such as Germany, Puerto Rico, and Taiwan. A recent result from the National Comorbidity Survey Replication Study conducted on about 10,000 people in the U.S.A has already suggested an adult prevalence rate of 4%.1, 2 Epidemiological studies revealed prevalence rates generally ranging from 4% to 12% in the general population of 6 to 12 years of age.6 According to the studies performed in our country and according to a research accomplished with a sample of 501 subjects, the prevalence of inattentive type among primary school children was 17.8%, the prevalence of hyperactivity was 13%, and the prevalence of the combined type was 6.2%.7 In a recent research performed on 400 subjects, the prevalence rate of ADHD has been reported as 9%.8 MATERIAL AND METHODS The Conners Parent Scale9, 10 (CPRS- 48) with five major elements of conduct problems, leaving problems, psychosomatics, impulsive-hyperactive and anxiety and also Conners Teacher Rating Scale11 (CTRS- 38) with six major elements of hyperactivity, conduct problems, emotional overindulgence, anxious-passive, asocial and day dream-attendance have been used in this research. Factor analysis method by using principal component method, factor matrix rotation with the help of equamax method, correlation method and student method have also been used in this research. This research includes two stages: the first stage is considering the prevalence of ADHD with cross-sectional survey and in the second stage the students who may have ADHD, will be semi-structurally interviewed. This section of the research is a type of descriptive study. For presenting the evidence of concurrence, validity/ reliability correlation coefficience between two CPRS and CTRS questionnaires were assessed. All students of primary schools in Tehran aged between 7-12 years, from 19 educational areas were our statistical universe, and a 2667 sample of boys and girls were selected for classification by stratified random sampling. Conduct problem scale can be concluded as below: cutoff 5 from the age of 6 to 8yr., cutoff 5 from the age of 9 to 11 yr. in learning problem scale, cutoff 3 in both from the age of 6 to 8yr. in psychosomatic scale and from the age of 9 to 11yr., in impulsive-hyperactive scale, cutoff 8 from age of 6 to 8yr. and cutoff 7 from the age of 9 to 11yr. in anxiety scale. RESULTS In the groups of 7-12 years of age, 8-year-old children with 588 instances and 12-year-old ones with 169 instances were the most and the least number of subjects respectively. In the study group of 1112 kids, 41% were the first child of their own families and totally 32% were the 3rd child of the family. Families with a single child were allocated about 51.4% of the total sample. Seventy seven percent of their mothers were housewives and 44% of their fathers had private jobs. The mean and standard deviation of the age of their mothers was 34 yr and 40 yr for the fathers. The scores of ADHD in 7 year old boys/girls in CPRS and CTRS were equal. The rates of the scores of ADHD in 8-year old boys/girls were equal, too. The scores of ADHD in 9-year-old boys/girls who have obtained the CPRS were equal. However CTRS showed that boys have higher ADHD scores than girls. There is no difference between the scores of the questionnaires of the boys and girls aged 10. Among all the 11 year old children, there were more boys than girls with ADHD. There is no difference among 12-year- old boys/ girls from the point of view of ADHD. According to the latest findings of both CPRS and CTRS of primary school children of Tehran aged between 7 to 12 years old, the prevalence of ADHD would be mentioned in a range of 3%- 6%. The mentioned findings compared to the following ones can be as the study (1999), and the announced statistics of APA (2003), declare that the prevalence of ADHD in children is about 3%- 5%. Although the average rate of ADHD in Brazilian children, along with research findings of Rohde studies (2005) may confirm this idea that its prevalence in boys is about 4% and it would not be confirmed for primary school boys, which its rate is about 19%.13 Therefore, as the results show, findings of the present study are consistent with the results of Conners and his colleagues studies; that is, prevalence of ADHD between 8-11 year-old children is much higher in boys than girls. From another point of view, since ADHD has co morbidity with conduct disorders, oppositional defiant disorder, learning disorder, depressive and anxiety disorders, it will make the clinical features more complicated and even the therapeutic responses will decrease. Therefore, special attention should be paid to diagnosis and treatment. However, the children with ADHD and their families are in great need of special short-term, intermediate and long-term national mental health systematic planning. CONCLUSION Our research has completely larified that ADHD is the most common psychiatric disorder in children. As ADHD causes significant impairment in family, academic and social functioning, early diagnosis and early intervention will prevent the consequences of ADHD. ACKNOWLEDGEMENT This research was supported by National Research Center of Medical Sciences of I.R. of IRAN. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06032f2.jpg] [mr06032t2.jpg] [mr06032t1.jpg] [mr06032t3.jpg] [mr06032f1.jpg] |
| |||||||||
{kind=link}
{kind=link}