 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
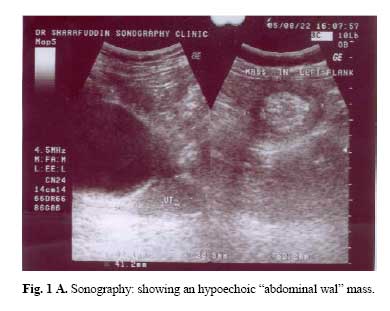
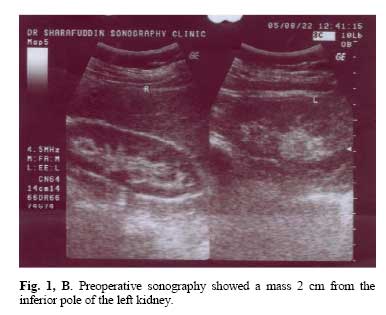
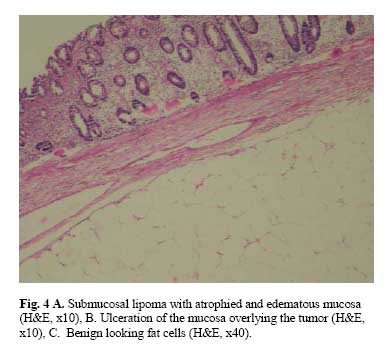
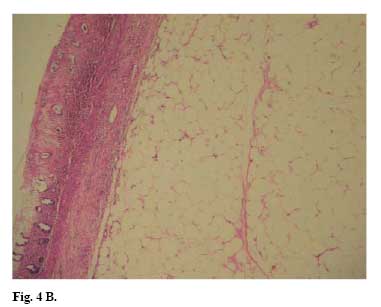
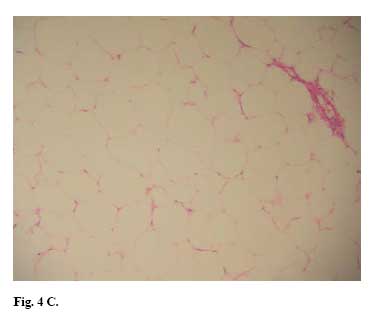
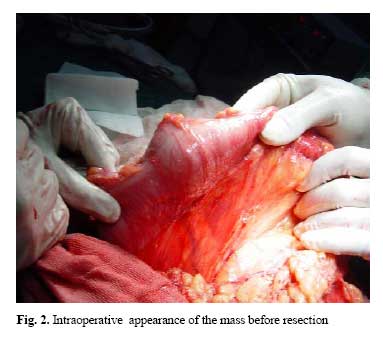
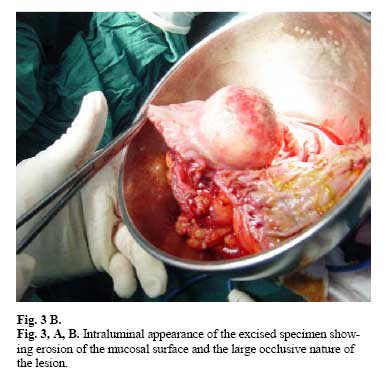
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 3, November, 2006, pp. 151-154 Case Report Colon Lipoma: A Case Report and Review of the Literature A.K. Motamedi, M.D.,* A. Dehestani, M.D., and M. Kadivar, M.D. From the Depts. of Surgery and Pathology, Hazrat Rasool Medical Complex, Iran University of Medical Sciences, Tehran, I.R. Iran. Code Number: mr06033 ABSTRACT Colon lipomas are rare. They are almost always asymptomatic; only when their diameter is more than 3 cm do they become symptomatic. They tend to occur in an older population and most of the cases are located at the right side of the large bowel. Usually the diagnosis is not made until operation is performed. We describe a 67-year-old woman with a large colonic submucosal lipoma causing left-sided abdominal pain and altered bowel habit. Abdominal sonography, CT scan and colonoscopy showed a mass 5 cm x 4.5cm x 4 cm located 90cm from the anal verge. Left hemicolectomy was performed, and histologic examination revealed the mass to be a benign colonic lipoma. We also reviewed the literature on the subject to examine the main characteristics of lipoma of the colon. Keywords: Colon, Lipoma INTRODUCTION Colon lipomas are rare and often asymptomatic, but large lipomas may produce abdominal pain, diarrhea, constipation, hemorrhage, and intussusception8. Since the symptoms and signs mentioned are not specific, it is difficult to make an accurate preoperative diagnosis. In lipomas less then 2 cm in diameter endoscopic removal is often possible, a surgical approach is recommended for larger lesions. CASE REPORT A 67-year-old woman was admitted to the general surgery department of our hospital for left-sided abdominal pain. She claimed she had this pain since 2 months ago. Her pain was persistent and was not related to food intake. She had an episode of bloody stools 2 weeks before admission and since then she had had loose bowel movements. She had lost weight but she didn't know its exact amount. She had a past medical history of asthma and hypertension. In abdominal examination, as the patient was relatively thin, a mass was palpated in the left lower quadrant. Digital rectal examination was normal. Detailed lab studies were all within normal limits, including complete peripheral blood cell counts, blood biochemistry and carcinoembryonic antigen levels. Fecal occult blood tests were done 3 times and were negative. Sonography of the abdomen, kidney and uterus was performed which revealed a mass (51mm x 41mm) outside the left kidney located 2 cm from its inferior pole with a hyperechoic central part (Figure 1a, b) but did not determine whether the mass was related to the colon. Abdominal CT scan revealed a mass with proximal fluid collection adjacent to the descending colon, however the exact location of the mass relative to the colon could not be definitively determined. Then the patient underwent colonoscopy and a round mass was seen 60cm from the anal verge which occupied the lumen almost completely and the colonoscope couldn’t pass through it. Several biopsies were taken and sent for histologic examination. Pathological examination showed mild chronic non-crypt destructive colitis. Finally the patient underwent laparotomy. Left hemicolectomy was done and the resected section was sent for pathologic studies. The lumen of the excised colon was opened intraoperatively revealing a round mass (5cm x 4.5cm x 4cm) with a cream-brown surface.The cut surface of the mass was homogenous and yellowish with a soft consistency. A lymph node (6 x 5 x5 mm) was also present. In microscopic studies the lymph node didn't have any significant pathology but the mass had the characteristics of a benign lipoma (Fig. 4a, b, c). The patient had an uneventful postoperative course and was discharged after 5 days. DISCUSSION Lipomas occur throughout the intestinal tract with the colon having the highest incidence. They constitute the most frequent benign tumor of the colon and rectum after adenomas. Nevertheless they are uncommon.1 These lesions occur with the maximum frequency in the fifth or sixth decades of life and are mostly found in women. Most of them are located at the right side of the large bowel, accounting for nearly 90%of cases, an opposite distribution in comparison with adenocarcinomas and adenomatous polyps. In 10 percent of cases, the lipomas are multiple.2, 3 The most frequent type is the submucosal lipoma with a sessile or pedunculated appearance, and the remainder-are subserosal lipomas. They are almost always asymptomatic; only when their diameter is more than 3 cm do they become symptomatic. Their clinical symptoms are directly related to their size. The common symptoms of colonic lipomas include changes in intestinal rhythm, rectorrhagia, diarrhea, abdominal pain, occupation of the colonic lumen by the mass, or intestinal intussusception caused by the progression of the pedunculated lipoma.4 The spontaneous expulsion of a lipoma per rectum is an extremely rare phenomenon and may be in the form of a lump of hemorrhagic tissues defecated from the rectum due to self-amputation of the lipoma. Sometimes colon lipomas can also be the source of massive lower gastrointestinal bleeding.6 Since the symptoms and signs mentioned above are not specific, it is difficult to make an accurate preoperative diagnosis. Lipomas can also present in the form of multiple polyps in the colon. Some may exhipit atypical stromal cells and mimic malignancy. Lipomatosis of the ileocecal valve or other portions of the colon may be mistaken radiographically for a tumor. Considering the age and symptoms of these patients, malignant tumors are also a matter of concern. For the submucosal lipoma, colonoscopy may directly visualize the mass with tenting of the mucosa, which may be easily indented with a closed biopsy forceps. As the forceps are withdrawn, the tumor will soon spring back to resume its previous shape (pillow or cushion sign).7 The pressure exerted on the lesion may compress the superficial vessels and the distinctive yellow color of fat may be disclosed. Adipose tissue may protrude through the biopsy site (naked fat sign) which reveals the fatty characteristic of the tumor.9 Colonoscopic biopsy often cannot promote a diagnosis in cases of suspected lipoma, because the lesion is beneath normal mucosa; as in our case the result was nonspecific colitis. On the other hand biopsy increases the risks of bleeding and perforation. Computerized tomography is considered to be the definitive diagnostic measure in recognizing colon lipomas because the masses present a characteristic fatty densitometric value. On CT scan image, a lipoma has a uniform appearance with fat-equivalent density and a smooth border. But for small lipomas, the diagnostic value of CT is low.8 As fatty tissue is a poor conductor for electronic current, endoscopic removal of colon lipomas may cause complications and if the lesion is sessile or broadly-based the risk of perforation and hemorrhage is high.10 Surgical resection seems to be the ideal choice of treatment, especially when malignancy cannot be completely excluded. Colotomy and excision or segmental colon resection is recommended for complete removal of the lipoma when the diagnosis is definite. It is recommended to use laparoscopic or laparoscopically assisted methods for excision when feasible because the patient enjoys the benefit of complete surgical excision while foregoing the postoperative discomfort and morbidity of open celiotomy.11 If the preoperative diagnosis of colon lipoma can be made correctly, the extent of surgery may be appropriately limited. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06033f2.jpg] [mr06033f4a.jpg] [mr06033f3b.jpg] [mr06033f4c.jpg] [mr06033f3a.jpg] [mr06033f1a.jpg] [mr06033f1b.jpg] [mr06033f4b.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}