 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
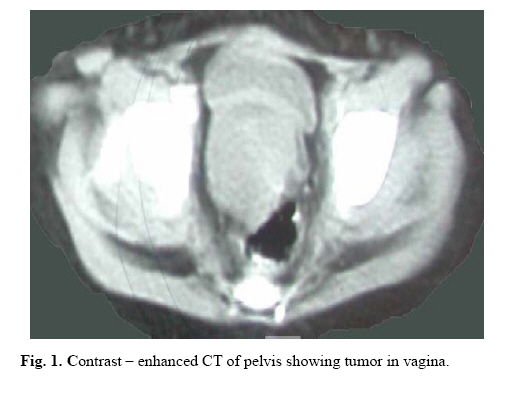
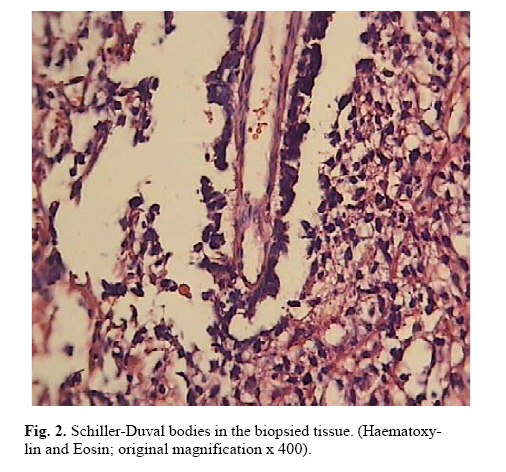
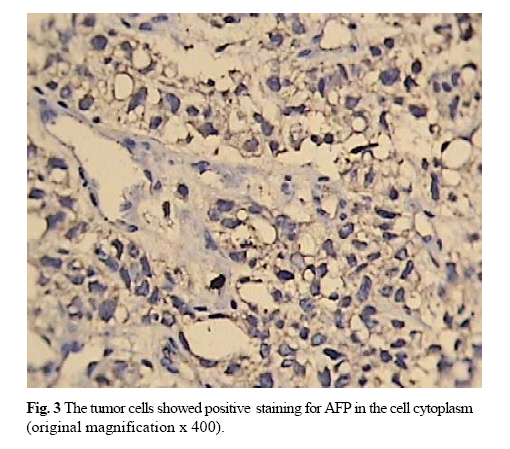
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 3, November, 2006, pp. 155-157 Case Report Yolk Sac Tumor of Vagina Parvin Mahzouni, M.D.,* Shervin Pejhan, M.D.,† and Mahmoud Ashrafi, M.D.† From the Dept. of Pathology, Alzahra Hospital, Isfahan University of Medical Sciences, Isfahan, Iran. Code Number: mr06034 ABSTRACT Malignant germ-cell tumors (MGCT) are rare tumors of childhood accounting for less than 3% of pediatric malignancies. Endodermal sinus tumor (EST) forms the most common histologic subtype of MGCT. The vagina is an extremely rare site for GCTs. An 8-month-old female was admitted with a short history of vaginal bleeding, and a mass protruding from the vagina. She was pale and a mass was palpable anteriorly on rectal examination. Computed tomography (CT) showed a tumor mass posterior to the bladder. A biopsy revealed a vaginal EST. The serum alpha-fetoprotein (AFP) was elevated. Vaginohysterectomy was done. The patient was subsequently referred to the oncologist for further management. EST is the most common GCT in children. In females, it is usually encountered in the ovary. EST of the vagina is a rare, highly malignant GCT that exclusively involves children less than 3 years of age. The diagnosis is based on histology and raised AFP. Vaginal EST is both locally aggressive and capable of metastasis. The serum AFP level is a useful marker for diagnosis and monitoring the recurrence of vaginal EST in infants. Keywords: Pediatric germ-cell tumor, Rare site, Vaginal endodermal sinus tumor INTRODUCTION Pediatric malignant germ-cell tumors (GCT) are rare tumors of childhood accounting for less than 3% of pediatric malignancies1. In children less than 3 years of age, the most common sites for GCTs are extragonadal and testicular.2 Endodermal sinus tumor (EST) is the most common histologic subtype of GCT.3, 4 We report an EST of the vagina, an extremely rare pediatric malignancy primarily affecting infants.5, 6 CASE REPORT An 8-month-old female was admitted with a history of bleeding per vagina of 1 month duration and protrusion of a mass from the vagina of recent onset. The child was apparently healthy until she developed vaginal bleeding. On examination the patient was pale. A mass was palpable anteriorly on rectal examination. Pelvic CT with and without contrast revealed a solid, cystic tumoral mass (4 x 3.5 x 3-cm), located anterior to the rectum, and at the posterio-superior aspect of the bladder (Fig. 1). There was no calcification or retroperitoneal lymphadenopathy. Contrast- enhanced computed tomography (CECT) did not show extension of the tumor beyond the vagina. A biopsy of the tumor mass showed tumor tissue arranged in a loose reticulum and microcystic areas lined by flat and cuboidal cells. Areas of hemorrhage and necrosis were observed. Festooning pseudopapillary processes with central vessels (Schiller-Duval bodies), and hyaline droplets were identified (Fig. 2). Immunohistochemical stain demonstrated the presence of AFP in the tumor cells (Fig. 3), and a diagnosis of vaginal EST was made. Serum alpha- fetoprotein (AFP) was elevated at 926 ng/ml. The patient was taken to surgery, where a vaginohysterectomy was done. The tumor was arising from the superior part of the vagina. Uterus and cervix were free of tumor, and there was no infiltration into the bladder and rectum. Gross appearance of the tumor was that of a pale tan-yellow slimy tumor with foci of necrosis. Microscopically, the biopsy findings of yolk sac tumor were confirmed. The patient had a smooth postoperative recovery and was referred to the oncologist for further management including combination chemotherapy. She will be followed up with AFP level estimation and CT scan when necessary. DISCUSSION EST is the most common GCT in children. In females, it is usually encountered in the ovary.7 EST of the vagina is a rare, highly malignant GCT8 that exclusively involves children less than 3 years of age.8, 9 The clinical presentation includes a history of bloody vaginal discharge, often accompanied by a polypoid mass protruding from the vagina. A vaginal examination under anesthesia is the best way to diagnose a yolk sac tumor of the vagina.10 Sarcoma botyroides - a variant of embryonal rhabdomyosarcoma - is the most common differential diagnosis. It is a common vaginal tumor of infancy and presents with vaginal bleeding and a mass. However, it has a characteristic grape like appearance and there are edematous and cellular areas formed of immature skeletal muscle cells which help in distinguishing it from a yolk sac tumor. Formerly, yolk sac tumor of the vagina was confused with a clear cell carcinoma of the vagina. However, the former has always occurred in children less than 3 years of age and later has not been reported at that young age. The histopathological examination confirms the differentiation between the two. Alpha-fetoprotein level in blood is usually elevated at presentation and should be used as guide to monitor therapy as well as detect a recurrence.11 The histologic diagnosis of EST is based on the finding of Schiller-Duval bodies, as was demonstrated in our case. The usefulness of monitoring serum AFP in the patients with EST is well established.12 In our case the serum AFP was checked after histological diagnosis as the first clinical and radiological diagnosis, based on the site of the tumor was sarcoma botyroides. In patients suspected of having vaginal EST, elevated serum AFP is a diagnostic tumor marker that can be used to monitor the course of the disease.13 To conclude, we emphasize on the need for complete evaluation of infants presenting with painless vaginal bleeding. As the source of blood found in diapers of young girls without overt cause is uncertain, one should maintain a high index of suspicion for any potential underlying pathological condition. Apart from radiological investigations as diagnostic tools, one might consider measuring AFP in such patients. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06034f1.jpg] [mr06034f3.jpg] [mr06034f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}