 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Volume 57, Number 7, July 2003, pp. 294-299 Imipenem resistance in nonfermenters causing nosocomial urinary tract infections N Taneja, S MAharwal,* M sharma,** Assistant Professor; *Ph.D student; **Professor & Head, Department of
Medical Microbiology, PGIMER, Chandigarh 160012.
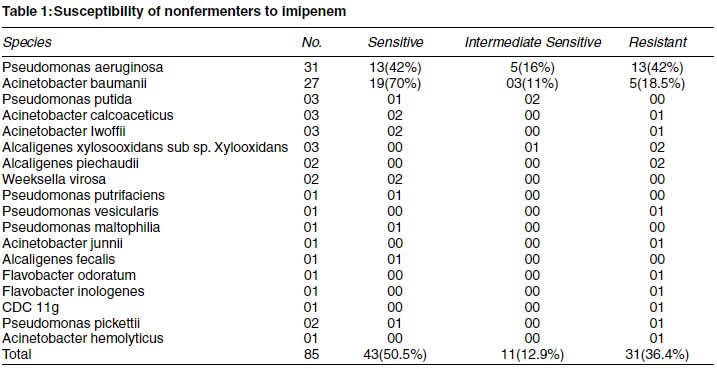
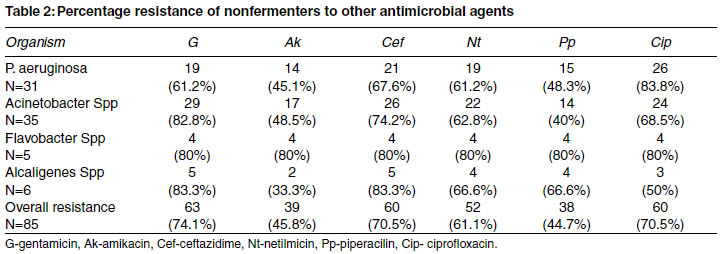
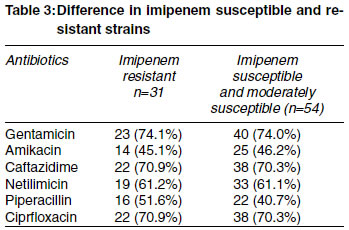
Code Number: ms03003 INTRODUCTION Nonfermentative gram-negative bacilli (nonfermenters) are generally saprophytic in nature but can cause a significant number of infections, particularly in the hospitalised patients and compromised hosts. Pseudomonas aeruginosa and Acinetobacter baumanii are most common nonfermenters pathogenic for humans. Infections caused by other species are relatively infrequent.1 Antimicrobial treatment of the nosocomial infections caused by these agents may be compromised by multiple drug resistance to β-lactams, aminoglycosides and fluoroquinolones.2,3 Imipenem, a broad spectrum β-lactam antibiotic and the first carbapenem to be used for clinical use, is an important drug for treatment of such infections. Imipenem offers the advantage of being more stable to most β-lactamases than the third generation cephalosporins.4 Unfortunately paralleling its increasing use in the west, resistance to imipenem has increased mainly among gram negative bacilli and particularly P. aeruginosa.4,5 In the SENTRY Antimicrobial Surveillance program (SASP), 10 to 30% of P. aeruginosa strains from various countries have been found to be resistant to imipenem. The nosocomial strains of nonfermenters exhibited a higher level of resistance. Though imipenem is not yet licensed in India, it is being used in the treatment of complicated infections not responding to other antimicrobial agents. To the best of our knowledge, no published data is available as far as resistance to this drug in nonfermenters is concerned. Therefore, the present study was undertaken to find out the minimum inhibitory concentration (MIC) of imipenem for nonfermenters causing nosocomial UTI, to study the antibiotic resistance to other antimicrobial agents and to compare the difference in antibiotic susceptibility among imipenem sensitive and resistant strains. MATERIAL AND METHODS Test organisms : A total of 85 strains of nonfermenters isolated in pure culture and significant numbers from same number of patients suffering from nosocomial urinary tract infections were taken up for the study. The strains were identified and characterized by the following tests: gram strain, oxidase test, catalase test, motility both by hanging drop as well as semisolid agar method, citrate utilization, urease production, hemolysis on 5% sheep blood agar, growth in 6.5% NaCl, ability to grow on MacConkey's agar, nitrate reduction, pigment production, indole production, lysine and ornithine decarboxylation, arginine dehydrolase test, growth at 4°C and 42°C, oxidation of 1 % glucose, xylose, lactose, maltose, sucrose and mannitol in Hugh Leifson's medium, susceptibility to penicillin (10U) and polymyxin (3000). The identification was done as per the manual for identification of nonfermenters.7 The media were obtained from HiMedia laboratories, Bombay (India). Antibiotic Sensitivity : Antibiotic sensitivity was done by the disk diffusion method of modified Stokes.8 The Strains were tested against gentamicin (10µg), amikacin (100µg), ceftazidime (30µg), piperacillin (100µg) and ciprofloxacin (5µg). P. aeruginosa NCTC 10662 and E. coli NCTC 10418 were used as the control organisms. Antibiotic discs were obtained from HiMedia laboratories, Bombay (India). Minimum inhibitory concentration of Imipenem : (Merck, Sharp and Dohme Co) was done by the agar dilution method. Briefly Mueller - Hinton agar plates with the following concentrations of the antibiotic were prepared 1,2,4,8,16,32,64 & 128 µg/ml. The strains were incubated overnight into the Mueller - Hinton broth. Next day the turbidity was adjusted to 0.5 McFarland and the broths were diluted 1:100 to give an inoculum of 104colonies/10µ spot. The plates were incubated overnight at 37°C. P. aeruginosa NCTC 10662 and E. coli NCTC 10418 were used as control strains. Isolates were classified as either resistant (R) (MIC > 16µg/ml) or susceptible (S) (MIC < 4 µg/ml) or intermediately sensitive (IS) if MIC was 8 µg/ml. Statistical analysis : Statistical analysis was done by applying Chi-square test. RESULTS The 85 strains included Pseudomonas spp. (39); Acinetobacter spp (35); Alcaligenes spp (6), Flavobacter spp (2), Weeksella virosa (2) and one strain of CDC IIg. Overall 36.4% of the strains were resistant (R) and 12 % were intermediately sensitive (I S) to imipenem. Forty-two percent of P. aeruginosa and 18.5% of Acinetobacter baumanii were imipenem resistant. Other strains which were resistant to imipenem included Alcaligenes spp (4/6), Acinetobactercalcoaceticus (1/3), Acineto-bacterlwoffi (1/3), Acinetobacterhemolyticus (1/1), Acinetobacterjunii (1/1), Burkholderia (Pseudomonas) pickettii (1/2), Burkholderia vesicularis (1/1), CDC IIg (1/1) and Flavobacter odoratum (1/1) and Flavobacter indologenes (1/1) (Table 1). The table 2 depicts the percentage resistance to other antimicrobial agents. A high level of drug resistance was observed (>70% for ceftazidime, gentamicin and ciprofloxacin). Least resistance was observed for piperacillin and amikacin (approximately 45% each). Seven out of 31 strains were multi drug resistant. P. aeruginosa (MDR PSA- defined3 as P. aeruginosa resistant to gentamicin, piperacillin, ceftazidime and imipenem). The difference in the antibiotic susceptibility to other agents among the imipenem susceptible (n=54) and imipenem resistant (n=31) is depicted in table 3. The difference was not statistically significant even for piperacillin. DISCUSSION Nonfermenters are ubiquitous in the environment. Usually considered as contaminants they have emerged as important nosocomial pathogens especially in immunocompromised hosts. These organisms cause a variety of infections including UTI,9,10 ( Antibiotic resistance is a major clinical problem in treating infections caused by these microorganisms. A combination of a β-lactam agent and an aminoglycoside has most commonly been used for treatment especially the ones caused by P. aeruginosa;9,11 Other antibiotics which have been used are fluoroquinolones.7,8 The resistance to the antimicrobials has increased over the years. Resistance rates vary from country to country.3,6 Overall, isolates from Latin American countries show the lowest susceptibility rates to all antimicrobial agents followed by Asian-Pacific isolates and European strains. Strains from Canada exhibit the best global susceptibility testing results. (SENTRY Antimicrobial Surveillance Program, SASP).3,6 The reported resistance (R) rates for P. aeruginosa in this program were as follows : ciprofloxacin (16 to 40%); piperacillin and ceftazidime (15 to 35%) and amikacin (3 to 31 %). Similarly, the resistance rates for Acinetobacter spp were ciprofloxacin (27 to 65.5%); piperacillin (23 to 72.9%); ceftazidime (19.8 to 65.6%) and amikacin (8 to 62.6%). The nosocomial strains from Latin American countries exhibited the maximum resistance.6 The results of our study are comparable to the situation in Latin America. Overall, approximately seventy percent of the strains were resistant to ciprofloxacin, ceftazidime, gentamicin and netimicin. Piperacillin and amikacin showed the best in vitro susceptibility pattern (approximately 45% R). These results are also comparable to those found in the SASP where amikacin had the best antimicrobial susceptibility profile. Apart from P. aeruginosa & Acinetobacter spp, Alcaligenes and Flavobacter also exhibited a high level of drug resistance to all the antibiotics. Least resistance was shown by other Pseudomonas spp. Imipenem is a carbapenem antibiotic, which is highly active against P. aeruginosa and Acinetobacter spp.1 This drug is highly β-lactamase stable and has an unusual property of causing a post antibiotic effect on gram negative bacteria.12 It is a small molecule, which can over come the poor outer membrane permeability of β-lactams for Pseudomonas by penetrating through the porin omp D2. Unfortunately paralleling its increasing use, resistance to this agent has also increased.5,9 The reported resistance varies from 10 to 30% in P. aeruginosa and 3 to 10.3% in Acinetobacter spp. In the present study overall imipenem resistance was 36.4%; the rates for P. aeruginosa and Acinetobacter baumanii being 42% and 18.5% respectively. Other nonfermenters showed variable resistances. Some like Alcaligenes exhibited high level of resistance (4 out of 6) and other Pseudomonas spp showed relatively less resistance (2 out of 8). In the present study, seven out of 31 strains of P. aeruginosa were MDR PSA resistant to piperacillin, ceftazidime, imipenem and gentamicin. Maximum numbers (8.2%) of these are reported from Latin America, followed by Europe (4.7%), Asia Pacific (1.6%), USA (1.2%) and Canada (0.9%).3 Apart from piperacillin, all other antibiotic exhibited the same resistance profile among the imipenem S and R isolates. However, this difference was not statistically significant. In the present study, the high level of drug resistance was most probably due to inclusion of strains causing complicated nosocomial infections. In fact, some of the patients failed treatment with 3 to 4 antibiotics. Piperacillin and imipenem either alone or in combination with amikacin were used for treating the patients not responding to treatment with fluoroquinolones, aminoglycosides and ceftazidime. More studies are required to know the exact magnitude of the problem in India. SUMMARY Nonfermenting gram-negative bacilli (nonfermenters) have emerged as important nosocomial pathogens causing opportunistic infections in immunocompromised hosts. These organisms show high level of resistance to β-lactam agents, fluoroquinolones and aminoglycosides. Imipenem is a carbapenem antibiotic, which can be very useful for treatment of infections caused by nonfermenters. Eighty-five nonfermenters causing nosocomial UTI were tesed for MIC to imipenem by agar dilution method. Resistance to other antimicrobial agents was compared between imipenem sensitive (S) and resistance (R) groups. Overall 36.4% of nonfermenters were resistant to imipenem. Forty two percent of P. aeruginosa and 18.5% of Acinetobacter baumanii were imipenem resistant. Other nonfermenters showed variable resistance, resistance in Alcaligenes spp. being very high. More than 70% of the nonfermenters were resistant to ceftazidime, gentamicin and ciprofloxacin. Piperacillin and amikacin had the best invitro susceptibility. No significant difference was found in the antibiotic susceptibility profile among imipenem sensitive (S) or resistant (R) strains. REFERENCES
Copyright 2003 - Indian Journal of Medical Sciences. The following images related to this document are available:Photo images[ms03003t2.jpg] [ms03003t3.jpg] [ms03003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}