 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Volume 57, Number 8, August 2003, pp. 338-346 COURSES OF SUBSTANCE USE AND SCHIZOPHRENIA IN THE DUAL-DIAGNOSIS PATIENTS: IS THERE A RELATIONSHIP? S Goswami, G Singh,* S K Mattoo,** D Basu*** Consultant Psychiatrist; *Assistant Professor; **Additional Professor; ***Associate
Professor, Drug
De-addiction and Treatment Centre, Department of Psychiatry, PGIMER, Chandigarh.
Accepted : 31-3-2003. Code Number: ms03011 ABSTRACT Background: Interrelationship of schizophrenia and substance use is complex and multifactorial. Examining the influence of various psychoactive substances on course of patients with dual-diagnosis schizophrenia may help to solve this riddle. Aim: To examine the relationship of the courses of substance use and schizophrenic symptomatology in substance abusing "dual-diagnosis" patients with schizophrenia. Settings and Design: Outpatient Deaddiction and Treatment Center of a tertiary care hospital with; retrospective design. Methods and Material: Twenty-two substance abusing dual-diagnosis patients with schizophrenia were investigated regarding the course of substance use (abuse/dependence, use, non-use) and that of schizophrenia (psychotic, non-psychotic, in remission). A graphical representation of course of schizophrenia and substance abuse was made and their relationship studied by superimposition of respective graphs. Statistics : The Friedman two-way analysis of variance of ranks was applied to see the relationship between time spent by patients while on and off various substances. Results: In five cases, the onset of schizophrenia preceded the onset of substance use. In seven out of 22 subjects, the schizophrenic exacerbation was clearly preceded by increase in substance abuse in the preceding 2-12 months. In none of the subjects decrease in substance use led to a decrease or increase in schizophrenic symptoms. Conclusions: Although substance use disorder preceded the onset of schizophrenic illness in the majority, and increase in substance abuse preceded schizophrenic exacerbation in one-third of dual-diagnosis patients, overall there was no evidence that the course of substance use was associated with that of schizophrenia after both disorders were diagnosed. Key Words: Schizophrenia, Course, Dual-diagnosis. INTRODUCTION Patients with co-existent mental illness and substance abuse are termed "dual-diagnosis patients" or `mentally ill chemical abusers or MICA'.1,2 Substance abuse among the patients with schizophrenia is an increasingly recognized problem,3,4 with 15-65% of schizophrenics reported to be using various substances.5,6 The substances of abuse such as LSD, cannabis and amphetamine have been reported to produce symptoms that mimic those of schizophrenia, thus confounding the diagnosis.7-9 These groups of patients are difficult to treat because of high relapse rates, poor drug compliance etc.1-3 They are likely to pose a burden to their families as well as to the societies to a greater extent than either a patient of substance abuse or schizophrenia alone.10 Psychoactive substances can also interact with the psychopharmacological agents used for the treatment of schizophrenia by directly counteracting their desired effects, by worsening their side effects profile or by altering their pharmacokinetic properties.11 All these variables in combination can alter the course of illness in both acute and chronic frames.10 The relations between drug abuse and schizophrenia can be of three types:12
Different researchers have tried testing these models in various studies. McLellan et al13 followed up 11 non-psychotic stimulant abusers over a six years period. Initially the `stimulants' included hallucinogens, amphetamines and inhalants, but at the end of six years, most patients were injecting amphetamine, methylphenidate, or both. In six of the 11 patients, a diagnosis of schizophrenia was made after the conclusion of six years of stimulant abuse. Andreasson et al14 studied a sample of male conscripts, who had given cannabis use history and undergone a screening for psychological disturbance at the age of 20 years. After 15 years, it was noted that schizophrenia was 2-4 times more likely to occur among the conscripts who had reported any use of cannabis at al, and that it was 6 times more frequent among men, who by the age of 20 years, had already used cannabis 50 times or more. Hence, the risk for schizophrenia increased as cannabis consumption increased. Few attempts have been made to test the second proposed relationship. Negrete et al15 found that schizophrenic patients who use marijuana reported an enhancement of psychotic symptoms. The suggested that the observed effects may be due to an exacerbation of psychotic symptoms or a secondary psychosis, superimposing on the schizophrenic state or, a diminution of the effectiveness of the antipsychotic medication. Hensala et al7 investigated the role of LSD in triggering psychotic episodes and hospitalizations. In 25% of the cases, LSD was directly related to the index hospitalization. In a 1-year prospective study of 93 schizophrenic patients, it was seen that 42% of cannabis abusing patients suffered a relapse as compared to 17% of non-cannabis abusing patients.8 When cannabis abusing groups were further divided into mild and severe, it was seen that 61% of heavy cannabis abusers suffered relapses as compared to 18% of mild cannabis abusers. In a follow up study, it was seen that contrary to majority of normal schizophrenic patients, the trajectory of symptoms of dual diagnosis patents changed from a predominantly negative to predominantly positive symptoms.16 Similar findings have been reported by Allebeck et al.17 Some evidence exists in favour of the third relationship. Zisook et al18 evaluated effects of previous alcohol and drug use on the course and symptoms of schizophrenia by comparing 34 patients with schizophrenia who had histories of substance abuse with 17 patients with schizophrenia who had no such history. It was concluded that there was no difference between the two groups. Davison19 did a review of LSD use in the United States and the Great Britain, in which the rate of prolonged psychosis (greater than two weeks) after LSD ingestion was not significantly greater than in the general population. From the existing literature, it is evident that equivocal evidence exists for all the three proposed relationships between schizophrenia and substance use. Literature is deficient on the account that no data is available on influence of various psychoactive substances on course of patients with pure dual-diagnosis schizophrenia. As the course of substance abuse is marked by remissions and relapses, no attempt exists to examine the relationship of this pattern of course with course of schizophrenia, which too is highly variable in same terms. There is no data available regarding the influence of substances such as opioids, alcohol, and cannabis (commonly used in India) on course of schizophrenia. The present study was hence planned as an attempt to examine the relationship of course of use of these substances with course of schizophrenia. MATERIAL & METHODS The study was conducted at the Drug De-addiction & Treatment Centre (DDTC), Department of Psychiatry of our Institute after obtaining necessary protocol clearance from the Thesis Committee of the Institute. Informed consent was obtained from the subjects before intake. The study sample comprised 22 male outpatients with schizophrenia and psychoactive substance abuse/dependence for at least a month preceding intake. The diagnosis of both schizophrenia and substance use disorder were made after history taking and clinical interview by SG/GDS of the patients and their relatives and/or other informants, according to the diagnostic guidelines as per the Diagnostic and Statistical Manual, 4th ed.20 The diagnoses were confirmed by further consultation with a consultant psychiatrist (DB/SKM). Other criteria were: For the index group, the schizophrenia syndrome presented either preceding substance abuse, or persisted for at least two weeks of substance-free state (in order to exclude potential cases of substance-induced psychotic disorders and to take only proper dual diagnosis cases).
After obtaining informed consent from the patients and/or their relatives, the following instruments were administered to consecutive patients attending our outpatient section and fulfilling all criteria for intake, in this order:
A graphical representation of course of schizophrenia and substance abuse was made and their relationship seen, for example, whether exacerbation of symptoms was associated with excessive use of drugs or not. The course of schizophrenic illness was divided into three parts or phases: Psychotic, Non-psychotic (though symptomatic), and Remission. Psychotic phase was said to be present when at least one of the following five symptoms was present.21
Non-psychotic symptomatic phase was said to be present when at least of the following 5 behaviours were noted.21
Remission phase was said to be present if following a psychotic episode, none of the symptoms listed as characteristics of a psychotic or non-psychotic episode was present for at least a period of 30 days or more.21 Substance use course was divided into i) abuse/dependence as per DSM-IV20; ii) use of substance, not diagnosable as above; and iii) non-use. For analysis the relationship between substance use and schizophrenic illness, the course of each was drawn separately on graph paper. Since, among the 22 substance-abusing schizophrenics there were three polysubstance abusers, there were 26 substance abuse graphs. For each case the course of schizophrenic illness and the course of substance were then compared by superimposition of respective graphs. The start point for comparison was the onset of the second disorder (schizophrenia, substance use disorder, or, at times when the onset was unclear, then both) since we were interested in that part of the illness since when the patient was truly `dual-diagnosis'. The end point for comparison was the date of study intake. The unit of comparison was: months spent by each patient in each phase of schizophrenia (psychotic, non-psychotic, and remission) and substance use disorder. It was seen that the substance abuse phase marked as "use of substance, not diagnosable as above (DSM-IV abuse/dependence)" was negligible compared with the time spent in either abuse/dependence or non-use; accordingly, for the purpose of course comparison, the months spent were actually counted under the dichotomous categorization of "on (particular substance)" vs. "off (particular substance)". Thus, for each patient and for a particular substance, there would be two substance use phases (months on drug, and months off drug) and three schizophrenia phases (months psychotic, months non-psychotic, and months in remission). STATISTICS Frequency and percentage, mean and standard deviation were used to describe demographic and clinical variables. For the course comparison, the non-parametric Friedman two-way analysis of variance of ranks was applied to the tables so generated separately for alcohol, opioids, and cannabis. RESULTS Sociodemographic profile Patients had a mean age of 33.5 years (SD, 9.44). Majority (55%) of patients were educated for more than ten years and employed as Un-/Skilled labourers (55%). Majority (55%) of patients were married and belonged to nuclear families (59%). Nineteen patients hailed from urban localities, and 55% of patients belonged to Hindu religion. Clinical profile Mean age of onset of schizophrenia in patients was 28.5 years (SD, 8.38) with mean duration of illness being 59.09 months (SD, 58.36); 17 out of 22 patients suffered from paranoid subtype of schizophrenia. Onset of illness was insidious in 20 patients. Eight patients had positive family history of schizophrenia and substance abuse. The substances used by the patients were as follows: opioids in 11 patients (codeine in four patients; pentazocine and dextropropoxyphene in two each; and buprenorphine, heroin and opium in one patient each); alcohol in nine patients; cannabis in five patients; and benzodiazepines in one patient. Three patients abused multiple substances; hence, the total number of substances (26) exceeded the number of patients (22). Course of illness From the visual inspection of the graphs, the following important findings emerged:
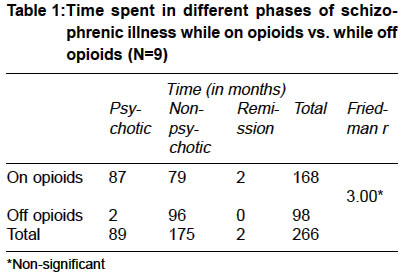
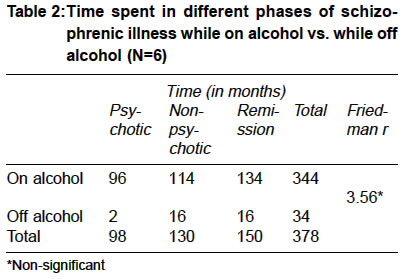
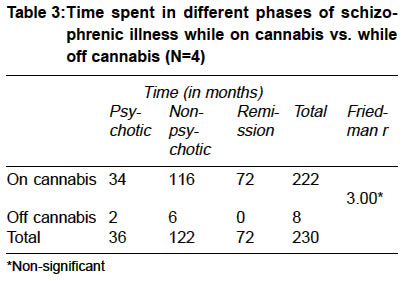
For the period when the schizophrenic illness and the substance use were co-existent, the analysis was done as mentioned before. Table 1 shows time spent in different phases of schizophrenic illness in opioid using patients while on opioids vs. while off opioids (N=nine). As shown in Table 1, the opioid-abusing schizophrenics, while taking opioids, spent more time in psychotic (87 months) and non-psychotic symptomatic phases (79 months) than in remission phase (two months). While off opioids, the patients spent more time in non-psychotic phase (96 months) than psychotic (two months) and remission phases (0 months). However the relation between three phases of schizophrenia and whether the patient was on or off opioids was not statistically significant. Table 2 shows time spent in different phases of schizophrenic illness while on alcohol vs. while off alcohol (N=six). As shown in Table two, the alcohol abusing schizophrenics, while on alcohol, spent more time in non-psychotic (114 months) and remission phases (134 months) than in psychotic phase (96 moths). While off alcohol, they spent 16 month each in non-psychotic and remission phases as compared to two months in psychotic phase. However, the relation between three phases of schizophrenia and whether the patient was on or off alcohol was not statistically significant. Table 3 shows the time spent in different phases of schizophrenic illness while on cannabis vs. while off cannabis (N=4). As shown in table 3, the cannabis-abusing schizophrenics, while on cannabis, spent more time in non-psychotic phase (116 months) than in remission (72 months) and psychotic phases (34 months). While off cannabis, patients spent more time in non-psychotic phase (six months) than in psychotic (two months) and remission phases (0 months). However the relation between three phases of schizophrenia and whether the patient was on or off cannabis was not statistically significant. DISCUSSION Relationship between substance abuse and its influence on symptomatology and course of schizophrenia is ideally investigated by prospective longitudinal follow-up of vulnerable substance abusers in order to test the vulnerability model as done in various studies. Similarly, to study the influence of substance use on relapses or exacerbation of psychosis, prospective longitudinal studies are essential and ideal. In dual diagnosis patients, these conditions are not always met. Hence, one may have to resort to retrospective data collection and attempting to draw conclusions by examining the relationship between various phases of schizophrenia and substance use. This is particularly relevant given the fact that both the illnesses have variable course punctuated by remissions and relapses. The present study with its limitations of being retrospective was an attempt to examine this relationship. Approach of superimposition of graphs indicating the course of two illnesses is the closest way one could have approached the "temporality" of two coexisting disorders. Most of the prospective studies have followed a cohort of patients and then stressed the increased vulnerability or substance abusers to psychotic episodes - an evidence for the vulnerability model.13,14 Our study design, being retrospective, could not directly test the vulnerability hypothesis. However, 17 out of our 22 patients developed substance use disorder prior to schizophrenia. This is at least in line with the vulnerability model. The case record studies along with semi structured interview of patients and relatives revealed that schizophrenic exacerbations were related to increase in substance abuse in seven out of 22 of cases, i.e., about one-third. This is in contrast to earlier findings where increase in substance use has been related to exacerbation of schizophrenic symptomatology.8,15 It could also be because the present study limited itself to studying patients using opioids, alcohol and cannabis rather than the psychostimulants studied in other studies. Hence, it may point to the need for examining the "psychotogenic" properties of these substances. This is reinforced by the fact that in no patient reduction of substance use led to reduction in symptomatology. Of course, this result should be interpreted cautiously because of a chance of retrospective falsification. Our study also compared the relation between various phases of schizophrenia and the course of substance use for the period when both were co-existent. The results did not show any statistically significant findings in any substances studied, though various trends were observed as mentioned before. It may mean that both substance use and schizophrenia exist independently in patients, neither influencing the course of the other, thus lending support to the third proposed relationship between the two. The negative findings could also be due to the small number of the sample. This type of study is possibly the first of its kind and needs to be replicated with large samples before any definitive conclusions can be drawn. Also, the results should not be generalized beyond our sample of male medicated outpatients with dual-diagnosis schizophrenia of predominantly paranoid subtype and with alcohol and opioids as the major substances of abuse. One advantage of this kind of a study design is that the patients serve as their own controls. Studies comparing course of schizophrenia in substance-abusing versus abstinent samples might actually be comparing different groups of patients as evidenced from the basic background differences apparent between the dual-diagnosis versus single-diagnosis patients in recent studies, such as in the areas of premorbid cognitive capabilities, gender, socioeconomic background, and clinical presentation, etc.22-24 These baseline differences, independent of substance-related influences, could fallaciously bear upon the course and outcome of the illnesses. Studying the same patients themselves through different phases of their illness would circumvent such fallacy. A second advantage of this design is to be able to study the relation of course of schizophrenia with different substances, since different substances may have different roles to play in the lives of patients with schizophrenia as we have explored recently.25 Thus, with a larger sample, even a retrospective design such as this can potentially generate useful data on the courses of these two disorders and their interrelation. Future work should progress in this direction. CONCLUSION In this small sample of outpatient male subjects with dual-diagnosis schizophrenia, although substance use disorder preceded the onset of schizophrenic illness in the majority, and increase in substance abuse preceded schizophrenic exacerbation in one-third, overall there was no evidence that the course of substance use was associated with that of schizophrenia after both disorders were diagnosed. REFERENCES
Copyright 2003 - Indian Journal of Medical Sciences. The following images related to this document are available:Photo images[ms03011t1.jpg] [ms03011t3.jpg] [ms03011t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}