 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Volume 57, Number 8, August 2003, pp. 347-349 Five year clinico pathological study of Breast Cancer A Goel, C M Bhan,* K N Srivastava** DA, MS; *M.S, FICS Consultant Surgeon; **MS, FICS, Department of Surgery,
Dr. Ram Manohar Lohia Hospital, New Delhi.
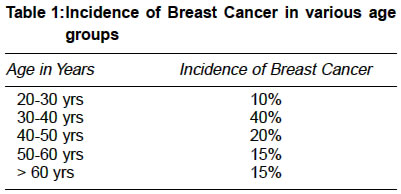
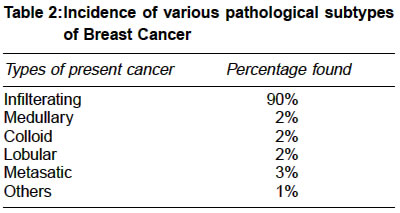
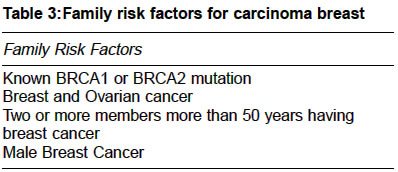
Accepted Date: 10-06-2003 Code Number: ms03012 ABSTRACT Breast cancer is a prototype for exploring variations in pathological diagnosis and etiology. BASIC PROCEDURE: We analysed the various risk factors, age, Tamoxifen treatment and pathological diagnosis for Breast cancer. MAIN FINDINGS: We present a review of 105 cases of breast cancers diagnosed and treated at Dr Ram Manohar Lohia Hospital in a five years prospective study between 1997and 2002. Breast cancer was most commonly found in age group 30-40 years and infilterating carcinoma of breast was the commonest occurring in 90% of the cases. IMPLICATIONS: We demonstrated the utility of such study of ensuring greater equity and understanding in etiology. The risk factors and pathological diagnosis in cancer of breast were studied and need for comprehensive screening programme were outlined. KEY WORDS: Breast cancer, Mammography, Screening, Tamoxifen. INTRODUCTION Breast cancer is a dynamic process and its increasing incidence in the last twenty years can be attributed to delayed child bearing, having fewer children and early detection. It has become one of the commonest female malignancies in our country. Early diagnosis, mammography screening and recognition of appropriate chemotherapy and hormonal therapy may reduce morbidity and improve survival.1 MATERIAL & METHODS We analysed about 105 cases of breast cancer being diagnosed and operated in our hospital between years 1997-2002. Mode of diagnosis was clinical examination, imaging, (ultrasound, mammography) and tissue diagnosis (Fine needle aspiration cytology, biopsy). After confirmation at tertiary level, all cases subjected to surgery and modified radical mastectomy (MRM) with or without axillary clearance was undertaken. Biopsy was sent for detailed histological diagnosis. Patients were later put on chemotherapy and hormonal therapy. Patients were some times downstaged with preoperative chemotherapy. We also studied the various etiological factors associated with breast cancer. CMF regime was given for chemotherapy. Radiotherapy was given as per indication. OBSERVATIONS We studied the age groups, social status, risk factors, Tamoxifen therapy and various pathological subtypes. Breast Cancer was most prevalent in age group of 30-40 years found in 40% of cases and most patients came from lower socio economic status. (Table 1) Average period for diagnosis was 2 months to 6 months. After routine diagnosis, surgery in form of MRM, simple mastectomy and lumpectomy were undertaken according to the diagnosis and spread of disease. Chemotherapy, radiotherapy was followed up with regular mammography in follow-up visits. Recurrence was reported in 5% of cases. The most common pathological diagnosis found in breast cancers was infiltrating duct cancer found in 90% of cases. (Table 2) It was found in most common age group of 30-40 years. DISCUSSION Randomized clinical trials have demonstrated that breast screening with mammography reduces cancer specific mortality.2 Recent cloning of two breast cancer susceptible genes BRCA1 and BRCA2 has now created possibility of predictive genetic testing (Table 3). It is the medically deprived population who do not have access to medical and academic research who are more likely to be detected for late stage breast cancer and bear greatest breast cancer risk.3 Breast cancer research states that disease free survival are better for patients attending screening programmes. Aldrich has also stressed the point of population base research and central cancer registries.4 Tamoxifen was an accepted adjuvant chemo-preventive agent along with chemotherapy and radiotherapy. It has been demonstrated in the clinical trials to be effective in reducing 50% incidence of breast cancer in survivors of the disease.5 Breast cancer prevention trial showed that Tamoxifen, a selective receptor modulator, reduces the incidence of breast cancer in healthy women, to be at high risk and after a mean follow up of 4 years Tamoxifen reduced incidence of breast cancer by 49% compared with a placebo.6 Ductal carcinoma is being diagnosed with increasing frequency and ductal carcinoma in situ of breast represents about 30% of all new cases.7 Hormonal replacement therapy is current used in about 38% in postmenopausal women in United States.8 Non modifiable risk factors include family history, age of woman at birth of first child, early menarche and late menopause. Potentially modifiable risk factors include alcohol consumption, use of postmenopausal hormones and obesity after menopause.9 Mammography is the best screening tool available and reduces cancer mortality and identifying cancer at an earlier stage. Individual assessment of breast cancer risk can be charted, women's medical care can be tailored to her risk. Breast cancer one of the common female malignancies has varied etiology and pathological status. The detection of breast cancer at an early stage with potential for cure should be a goal for all physicians. Our five year study analyses that age, Tamoxifen, pathological diagnosis have a direct bearing on the morbidity and mortality of disease. We propose that in order to increase the proportion of women who receive optional treatment, thus ensuring greater equity, a more sophisticated understanding of etiology and pathological variants is required. A comprehensive screening programme should include not only self examination of the breast and screening mammography but also risk assessment. Therapeutic treatment in clinical practice will be optimum if we understand these variations and detect the disease at earlier stage and reduce the mortality and morbidity associated with the disease. REFERENCES
Copyright 2003 - Indian Journal of Medical Sciences. The following images related to this document are available:Photo images[ms03012t1.jpg] [ms03012t3.jpg] [ms03012t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}