
|
Indian Journal of Medical Sciences
Medknow Publications on behalf of Indian Journal of Medical Sciences Trust
ISSN: 0019-5359 EISSN: 1998-3654
Vol. 57, Num. 10, 2003, pp. 442-449
|
Indian Journal of Medical Sciences, Volume 57, Number 10, October 2003, pp. 442-449
CORONARY ARTERY DISEASE INCIDENCE BETWEEN TYPE II DIABETIC AND NON-DIABETIC PATIENTS WITH LERICHE SYNDROME
Murat Özeren, Mehmet Kaya, Mustafa Kar, Ertan Yücel, Tahir Durmaz*
M.D.; Cardiovascular Surgery Department, Social Security Organization (S.S.K.) Ankara Education and Research Hospital Ankara, Turkey; *Cardiology Department, Specialization Hospital, Social Security Organisation, Ankara, Turkey
Correspondence:
Murat Özeren, MDKizilirmak cad 61/5, Kizilay, Ankara, 06640, Turkey.
E-mail: mozeren@yahoo.com
Accepted Date: 10-10-2003
Code Number: ms03029
ABSTRACT
Background: Coronary artery disease (CAD) is the major determinant
of preoperative morbidity and mortality for patients requiring major vascular
surgery. The management of CAD in these patients is controversial.
Aims: The
incidence and severity of CAD in diabetic and non-diabetic patients with Leriche
syndrome was explored.
Settings and design: 107 patients with Leriche syndrome
were selected as major vascular occlusion and grouped according to their diabetic
Status. Sex,
age, dyslipidemia, obesity, hypertension, clinic cardiac status, coronary angiographic
lesions and coronary revascularisation procedures were noted.
Material & Methods: Patients' demographics, intra-operative
and per-operative data were recorded and compared. In every patient with
Leriche syndrome scheduled for elective vascular reconstruction coronary
angiography was performed. Lesions were evaluated for the percentages of
stenosis. Preliminary coronary bypass or percutaneous coronary intervention
was recommended for those found to have advanced or severe CAD. Results of
revascularisation procedures were compared.
Statistical analysis used: Chi-square or Fisher exact chi-square
test is used for conditional variables. Independent samples was analysed
by using t-test. Kruskal-Wallis variance test was used if the variances are
not homogeneous according to the Levene test.
Results: No difference was found in both groups except family history and
obesity. Coronary angiographic investigation indicates that 59% of DIAB group
and 38% of NONDIAB group patients have advanced or severe CAD which has a
high probability for myocardial revascularization. Overall revascularisation
rate is 37.8% in DIAB group and 45.7% in NONDIAB group (p=0,641). Preoperative
mortality was found 2.7% in diabetics and 4.2% in non-diabetics (p=0.342).
Conclusions: Leriche syndrome with diabetes mellitus is
more likely to have advanced coronary disease than those without diabetes
mellitus. Coronary angiography and subsequent revascularisation should be
performed only in those patients who require major vascular surgery.
Key Words: Leriche syndrome, Coronary artery disease, Coronary angiography.
INTRODUCTION
Coronary artery disease (CAD) is the leading cause of morbidity and mortality following peripheral vascular reconstruction.1 The incidence of CAD in peripheral occlusive disease varies depending on series and selection of patients. In this study, Leriche syndrome as major vascular occlusion was selected for having a uniform group that can not be easily affected from the diabetic arteriopathy which mainly involves small and medium arteries. There is no consensus about the pre-operative management of CAD in patients with peripheral arterial occlusion. The physical limitations imposed by peripheral vascular disease may obscure the severity of coronary artery disease in these patients.2 Diabetes mellitus is the same risk factor for peripheral vascular and coronary artery disease and there is no report about incidence of CAD in Leriche syndrome with the coexisting diabetes mellitus. The purpose of this study is to evaluate the incidence and severity of CAD in diabetic and non-diabetic patients with Leriche syndrome.
MATERIAL & METHODS
Patient selection: Between October 1995 and August 2002, 107 patients
of Leriche syndrome were selected among 490 (21.8%) patients who were operated
for chronic occlusive aorto-iliac disease at the same period. Patients' demographics,
intra-operative and per-operative data were reviewed prospectively. Patients
with the following inclusion criteria were included in to the study: 1) All
patients had to be scheduled for coronary angiography or had to have a previous
coronary angiogram within 2 months of their participation in the study, providing
that no change in cardiac status. 2) Patients agreed to participate and signed
an informed consent approved by the ethical committee of Social Security Organization
(S.S.K.) Ankara Teaching and Research Hospital. Patients were excluded from
the study if they had undergone previous coronary bypass grafting or percutaneous
transluminal coronary angioplasty, had unstable angina, a recent (<6 months)
myocardial infarction, symptomatic valvular heart disease, congestive heart
failure and those requiring vascular operations on an urgent or emergent basis.
Patients with Leriche syndrome were divided into two groups as non-diabetic (NONDIAB) and diabetic (DIAB).
Peripheral vascular diagnosis
Claudication in one or both legs, possible decreased sexual potency in the male and diminished or absent femoral pulses; angiographically confirmed aortoiliac occlusion was defined as Leriche syndrome.
Diabetes Mellitus
Consistent elevation of fasting or 2 hour postprandial blood sugar level above 140 mg/dl, or abnormal glucose tolerance testing, either of which required formal management with insulin or hypoglycaemic agents was used as criteria of diabetes mellitus type II. Diabetic age was calculated by the extraction of first onset age of diabetes from the actual age of patient.
Dyslipidemia
According to the ATP III classification3 total cholesterol level above 240 mg% and LDL cholesterol above 160 mg % was accepted.
Hypertension
Patients with reproducible elevation of systolic or diastolic blood pressure above 140 or 90 mm Hg and who are requiring antihypertensive management to maintain normal blood pressure are accepted as hypertensive.
Obesity
Patients were considered obese if the body mass index (kg/m2) exceeded 20% of the ideal index.
Family History
Accepted positive if the patients' first degree male relatives had a coronary event at age <55 years or female relatives <65 years.
Clinical Cardiac Status
Cardiac history (previous myocardial infarction or angina pectoris, uncontrolled arrhythmia or congestive heart failure) and ECG changes (myocardial infarction, ischemic ST-T segment changes, and arrhythmia) were noted.
Cardiac catheterization
Coronary angiography and left ventriculography was performed to all patients prior to elective vascular reconstruction. Major coronary arteries were defined as the left anterior descending (LAD), circumflex (CX) and right coronary arteries (RCA). Diagonal and obtuse marginal branches were considered major vessels if they supplied a large enough area of myocardium. The extent of CAD was coded as 0,1,2,3 according to the narrowing of coronary artery (normal, <50%, 50-70 %,> 70). The results of the cardiac catheterisation were classified according to the following criteria4 : 1-Normal. 2-Mild to moderate CAD; measurable disease of one or more coronary arteries but no lesion exceeding 70% stenosis. 3-Advanced but compensated CAD; Greater than 70% stenosis of one or more coronary arteries but no immediate indication for myocardial revascularisation. 4-Severe, correctable CAD; Greater than 70% stenosis of one or more coronary arteries serving unimpaired myocardium and representing immediate or foreseeable risk for myocardial infarction. 5-Severe, inoperable CAD; Greater than 70% stenosis of multiple coronary arteries representing inadequate targets for coronary artery bypass grafting because of diffuse, distal disease or generalised ventricular impairment.
Statistical analysis
Data were collected and managed using a Microsoft Excel chart and analysed with SPSS for Microsoft Windows statistical analysis software. Analysis of these factors in NONDIAB group compared with DIAB group was performed by using chi-square or Fisher exact chi-square test for conditional variables. Independent samples were analysed by using t-test. Kruskal-Wallis variance test was used if the variances were not homogeneous according to the Levene test. Groups were bilaterally analysed with Mann-Whitney U test (with Bonforoni correction), if the significant differences were analysed by using Kruskal-Wallis variance test. A significant difference was assumed when p value was equal to or less than 0.05. Results are expressed as mean ± SD.
RESULTS
Sex and age
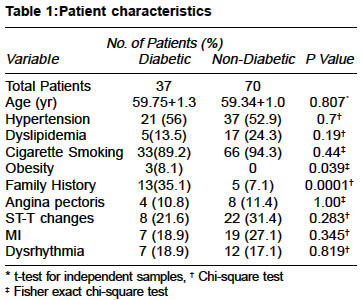
All patients were male in DIAB and NONDIAB groups. Age of diabetic patients were 59.75±8.05, ranging between 44 and 80 years and non-diabetic patients were 59.34±8.43, ranging between 33 and 73 years (p=0.807).
Cholesterol levels, Hypertension, angina, ST-T changes, myocardial infarction dysrhythmia, and ASA classification were found to be nonsignificant. Family History (p=0.0001) and Obesity (p=0.039) were found significant in favour of DIAB group. Patient characteristics were outlined in table 1.
The mean diabetic age of the patients was
5.29± 0,81 ranging between 4.6 and 6.6 years. Diabetic age was the highest in three vessel involvement group and significantly high involvement was found in the right coronary artery (p=0.021).
Angiographic classification of CAD
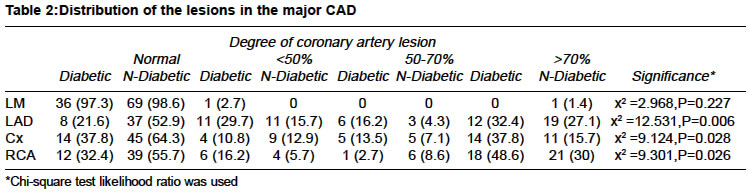
Major coronary artery involvement was compared with the chi-square likelihood ratio. LAD (c2 =12.531,p=0.006), Cx (c2 =9.124,p=0.028) and RCA (c2 =9.301,p=0.026) involvement was found significant in DIAB group. Distributions of the lesions in the major CAD were shown in table 2. Significance was not found in the comparison of ejection fraction (EF) and left ventricle wall dysfunction ( LV) in both groups (p=0.540).
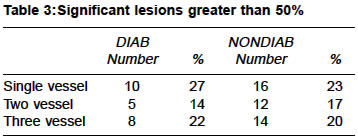
Employing greater than 70% stenosis as the criterion, significant CAD involved a single vessel in 10 (27%), two vessels in 5 (14%), three vessels in 8 (22%) in DIAB group and single vessel in 16 (23%), two vessels in 12 (17%), three vessels in 14 (20%) were found in NONDIAB group (table 3).
Clinic and angiographic distribution
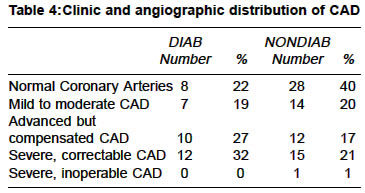
The clear distinction between the results of coronary angiography and clinic manifestations between DIAB and NONDIAB groups is shown in table 4. A normal coronary system or mild to moderate CAD was found in 15 (41%) and 44 (60%) of these groups, respectively. Advanced but compensated CAD was found in 10 (27%) patients in DIAB group and in 12 (17%) patients in NONDIAB group. Severe, correctable CAD was found in 12 (32%) patients in DIAB group and in 15 (21%) in NONDIAB group. While inoperable CAD was present only in one patient in NONDIAB group.
Ventricular Function
Normal ventricular function was found in 67.6% of patients in DIAB group and 70% of patients in NONDIAB group. Segmental akinesia in the distribution of previous infarction was found in 32.4% of patients in DIAB group and 30% of patients in NONDIAB group. Any significance was found in both groups (c2 =0.067,p=0.796).
Pre-operative revascularisation
Percutaneous coronary intervention (PCI) was performed on 15 (21%) patients in NONDIAB group and 3 (8.1%) patients in DIAB group. Coronary artery bypass grafting (CABG) was performed on 17 (24%) patients in NONDIAB group and 11 (29%) patients in DIAB group. Overall revascularisation rate is 37.8% in DIAB group and 45.7% in NONDIAB group (p=0,641). Vascular reconstruction was done three months after CABG and 3 to 4 weeks after PCI.
Peri-operative cardiac mortality was occurred
in one (2.7%) CABG performed patient
in DIAB group and 3 (4.2%) patients (1 PCI and 2 CABG) in NONDIAB group
(p=0.34).
DISCUSSION
CAD and MI are the most important reasons for peri-operative mortality and morbidity in patients with peripheral vascular disease in different series.5,6 Nowadays, better pre-operative assessment with the use of ergometric tests, myocardial nuclear scans, echocardiography and dobutamine stress echocardiography, and rational use of invasive techniques are decreasing the mortality and the morbidity.
CAD is the principal cause of death in patients with diabetes mellitus. The Framingham study documented that cardiovascular disease is two to three times more common in patients with diabetes than that would be expected for the population as a whole.7 The presence of CAD and MI may go undetected in diabetes, however, because the classic manifestations of chest pain associated with cardiac ischemia and MI may be absent because of associated autonomic neuropathy.8 Because silent MI and infarction is particularly common in patients with diabetes.9
Some authors thought that routine
coronary angiography and prophylactic myocardial revascularisation before vascular surgery is
not practical. The reported prevalence of CAD in patients with peripheral vascular
disease varies from 16 to 92 percent.10 The correct approach for the management of major vascular operations remains controversial. Several non-randomized and uncontrolled studies have suggested that coronary bypass surgery before a peripheral vascular procedure can reduce the likelihood of myocardial infarction and cardiac death after the peripheral vascular operation.11,12
The present report of 107 patients is an attempt to classify the incidence of advance and severe CAD so that coronary angiography may be employed routinely. The results of this investigation indicate that 59% of DIAB group and 38% of NONDIAB group patients scheduled for lower extremity revascularisation have advanced or severe CAD which has a high probability for myocardial revascularization. In this series, 14 of 22 (63%) patients of DIAB group and 32 of 37 (86%) patients of NONDIAB group with advanced or severe CAD had a myocardial revascularisation.
The Cleveland Clinic study showed that 1000 patients with peripheral vascular disease who underwent coronary angiography, only 8 % had normal coronary arteries, 60 % of patients had coronary artery stenosis greater than 70 %, and furthermore 25 % had severe CAD amenable to surgery.4 The percent of normal coronary artery (22% DIAB and 40% NONDIAB) and the rate of revascularisation (37% of DIAB group and 45.7% of NONDIAB group) in our study were found higher than this report.
Prevalence rate of 3 vessels CAD (22% diabetic vs 20% non-diabetic) was found similar in the recent study of Sukhija et al.13 In their study, higher prevalence of left main CAD (18% vs <1%), a higher prevalence of 3- or 4-vessel CAD (63% vs 11%), and a higher prevalence of obstructive CAD (98% vs 81%) was found in the coronary angiographic comparison of patients without peripheral arterial disease and with peripheral arterial disease for suspected coronary artery disease.13
So far, the beneficial effect of CABG in reducing the risk of peri-operative cardiac complications has only been addressed in retrospective studies. The largest retrospective review to date, based on the study population of the Coronary Artery Surgery Study (CASS) registry suggests that CABG has a beneficial effect prior to non-cardiac surgery.14 There was a substantial reduction in peri-operative mortality (1.7% vs 3.3 %) who had gone prior CABG, compared to those managed medically.
There are no controlled trials comparing peri-operative cardiac outcome after non-cardiac surgery for patients treated with pre-operative PCI versus medical therapy but observational data suggest that cardiac death is infrequent in patients who have undergone PCI before non-cardiac surgery. Peri-operative mortality of our group was higher then CASS registry. The reason of this high mortality rate is that the Leriche syndrome as major vascular disease has a complex surgical procedure than the other vascular procedures.
The present study confirms that patients with Leriche syndrome with diabetes mellitus are more likely to have advanced coronary disease than those without diabetes mellitus, but clinical cardiac status is more closely correlated with the incidence of severe, correctable CAD than the presence of diabetes mellitus alone.
Cardiac risk stratification in patients scheduled for major vascular surgery such as Leriche syndrome may facilitate the use of Peri-operative risk reduction strategies. Coronary angiography and subsequent revascularisation should be performed only in those patients who require major vascular surgery.
ACKNOWLEDGEMENTS
We would like to thank for the statistical analysis of this paper to Ilker Etikan Ass. Prof. from Hacettepe University School of Medicine, Department of Biostatistics.
REFERENCES
- Kertai MD, Poldermans D, Bax JJ, Klein J, Van Urk H. Cardiac risk and
perioperative management. J Cardiovasc Surg 2003;44:431-5.
- Hertzer NR, Young JR, Framer JR, et al. Coronary angiography prior to elective
aortic reconstruction. Results of selective myocardial revascularisation
in patients with peripheral vascular disease. Arch Surg 1979:114:1336-44.
- Talbert RL. Role of the National Cholesterol Education Program Adult treatment
panel III guidelines in managing dyslipidemia. Am J
Health Syst Pharm 2003;60:3-8
- Hertzer NR, Beven EG, Young JR, et al. Coronary artery disease in peripheral
vascular patients. A classification of 1000 coronary angiograms and results
of surgical management. Ann Surg 1984:199;223-33.
- Krupski WC, Layug EL, Reilly LM, Rapp JH, Mangano DT. Comparison of cardiac
morbidity between aortic and infrainguinal operations. J Vasc Surg 1992;15:354-65.
- Gajraj H, Jamieson W. Coronary artery disease in patients with peripheral
vascular disease. Brit J Surg 1994;81:333-42.
- Garcia MJ, McNamara PM, Gordon T, Kannel WB. Morbidity and mortality in
diabetics in the Framingham population: sixteen-year follow study. Diabetes
1974;23:105-11
- Niakan E, Harati Y, Rolak LA, Comstock JP, Rokey R. Silent myocardial infarction
and diabetic cardiovascular aotonomic neuropathy. Arch Intern Med 1986;146:2229-30.
- Chiariello M, Indolfi C, Cottechia MR, Sifola C, Romano M, Condorelli M.
Asymptomatic transient ST changes during ambulatory ECG monitoring in diabetic
patients. Am Heart J 1985;110:529-34.
- Gajraj H, Jamieson W. Coronary artery disease in patients with peripheral
vascular disease. British Journal of Surgery 1994;81:333-42.
- Crawford ES, Morris GC Jr, Howell JF, Flynn WF, Moor head DT. Operative
risk in patients with previous coronary artery bypass. Ann Thorac Surg 1978;76:215-21.
- Toal KW, Jacocks MA, Elkins RC. Preoperative coronary artery bypass grafting
in patients undergoing abdominal aortic reconstruction. Am J Surg 1984;148:825-9.
- Sukhija R, Yalamanchili K, Aronow WS. Prevalence of left main coronary
artery disease, of three- or four-vessel coronary artery disease, and of
obstructive
coronary artery disease in patients with and without peripheral arterial
disease undergoing coronary
angiography for suspected coronary artery disease. Am J
Cardiol 2003;92:304-5.
- Eagle KA, Rihal CS, Mickel MC, Holmes DR,
Foster ED, Gersh BJ. Cardiac risk of
noncardiac surgery: influence of coronary disease and
type of surgery in 3368 operations. Circulation 1997;96:1882-7.
Copyright 2003 - Indian Journal of Medical Sciences.
The following images related to this document are available:
Photo images
[ms03029t3.jpg]
[ms03029t1.jpg]
[ms03029t2.jpg]
[ms03029t4.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}