 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Volume 57, Number 10, October 2003, pp. 450-456 Socioeconomic Burden of Nosocomial infections Ata Nevzat Yalcin* *Akdeniz University, School of Medicine, Dept. of Infectious Diseases & Clinical Microbiology, Antalya, Turkey Correspondence:
Prof. Dr. A. Nevzat Yalcin, Akdeniz Universitesi, Týp Fakultesi, Infeksiyon Hast. & Klinik Mikrobiyoloji AD 07050, Antalya,Turkey. Accepted Date: 23-09-2003 Code Number: ms03030 ABSTRACT Nosocomial infection represents an important public health problem in developing countries as in developed ones. Economic concerns have taken on increasing importance in infection control since the mid 1970s in the USA, however there are few papers on the economics of NI in other countries. Studies on the costs of NI have used different methods, definitions and degrees of stringency when calculating indirect costs and there is therefore still uncertainty over their true economic impact on the community and on the workplace economy. Drug and especially antibiotic acquisition in addition to increased length of stay are the widely and well described parameters. Extra cost of NI include; bed, intensive care unit stay, hematological, biochemical, microbiological and radiological tests, antibiotics, other drugs, extra surgical procedures and working hours. In addition to high morbidity and mortality one of the well described parameters is the extra length of stay in the hospital. High mortality rates and economic expense which NI represents emphasizes the justification for measures of control of this entity. To estimate better the current personnel and financial resources necessary to support infection control activities and to prevent NI, it is imperative that those conducting studies of hospital epidemiology and healthcare outcomes research determine these current costs. Key Words: Nosocomial infection, Cost, Morbidity, Mortality. Approximately 5% of hospitalized patients experience a Nosocomial infection (NI). NI represent an important public health problem in developing countries as in developed ones today as a major cause of high morbidity, mortality and economic consequences in hospitalized patients.¹ In United States of America (USA) it is estimated that over two millions of NI occur annually with an extra cost of $ 4 billion and causing 80 000 deaths.² In England it is estimated that there are at least 100 000 cases of NI causing 5000 deaths each year with an annual extra cost estimated about £ 930 million (1.6 billion Euros).³ Economic concerns have taken on increasing importance in infection control since the mid 1970s in the USA, however there are few papers on the economics of NI in other countries. Substantial progress has been made in recent years to improve infection control in countries with limited resources, including national initiatives in Asia and Latin America. Changes in approaches to management in the health service with a greater requirement for accountability mean that there is now an increased need for costing studies.4 There are effective interventions for reducing the occurrence of NI, but like many events in complex systems, they require changes throughout the hospital and come with substantial costs. The techniques of economic evaluation have now been widely applied in health care. These techniques assess the value for money from interventions by comparing their costs and consequences. Economic evaluation consist of different analysis methods. In the field of NI control there are examples of economic evaluation based on a randomized clinical trial, or on synthesis of clinical evidence from a number of studies; this to be encouraged. Controlled study is required not only for assessment of clinical outcomes but also for the economic outcome.5,6 In estimates of hospital numeration, hospitals receive additional payments that account for only 1 % to 5 % of the actual costs of care to deal with NI.6 In calculating the cost of NI there are different methodological subjects;
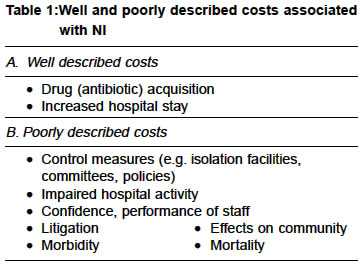
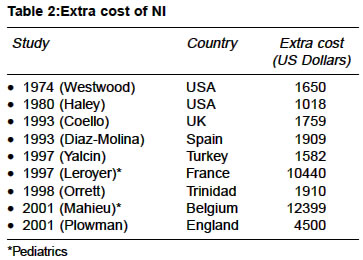
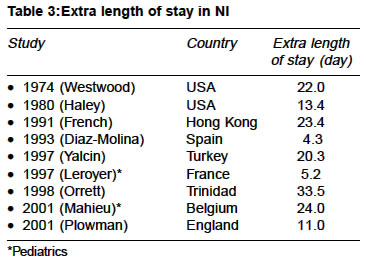
Studies on the costs of NI have used different methods, definitions and degrees of stringency when calculating indirect costs and there is therefore still uncertainty over their true economic impact on the community and on the workplace economy. Drug and especially antibiotic acquisition in addition to increased length of stay are the widely and well described parameters. However; control measures, impaired hospital activity, litigation, morbidity and attributable mortality are poorly described (Table 1).7 EXTRA COST Extra cost of NI include; bed, intensive care unit stay, hematological, biochemical, microbiological and radiological tests, antibiotics, other drugs, extra surgical procedures and working hours. Extra cost of NI varies between $1000-45003,8-13 with a mean $1800 (6), but in pediatric patients especially in neonatal units extra costs over $10.000 are reported (Table 2).14,15 Prolongation of hospital stay is the major extra cost attributable to NI in the US.16 In some studies cost of antibiotics are approximately half of the whole expenses.12 Although extra hospital days were reported as a major socioeconomic consequence of NI in many studies, extra costs due to antimicrobial treatment of NI analysed by site pathogens and drugs have not been widely reported until now.16 To calculate the true costs of antibiotic therapy, hidden costs arising from intravenous administration, labor, serum antibiotic assay, monitoring of hematological and biochemical indices and adverse effects of antibiotics must be considered. Therapeutic failures attributable to inappropriate antibiotic usage and poor bioavailability increase the costs. An estimate of the daily antibiotic cost of NI was made in France in 1996; resulting in 103 to 216 French Franks per infected patient.16 In a similar study by Yalcin et. al. in Turkey,17 daily antibiotic cost was described for systems; the least cost was found for urinary tract infections ($47.3) and nosocomial pneumonia had the highest costs ($90.3). Daily antibiotic cost for various microorganisms varied between $48.5 and $111.7. The estimated average costs of these infections are $593 to $700 for each urinary tract infection, $690 to $2734 for each surgical site infection, $4947 for each pneumonia, and $3061 to $40000 for each bloodstream infections.1,6 EXTRA LENGTH OF STAY In addition to high morbidity and mortality one of the well described parameters is the extra length of stay in the hospital. The comparative method matches NI cases with comparable non-infected controls, and is generally the favoured approach. Patients matched with controls are taken into to studies. Gender, age, underlying diseases, patients' clinic are used in matching process.9,10,18 Extra length of stay is reported about 433.5 days in different days (Table 3).3,8,9,11-16,18,19 The excess duration of hospitalization secondary to bloodstream infections, surgical site infections, urinary tract infections and ventilator-associated pneumonia is reported as 7-21 days, 7-8 days, 1 day and 6 days respectively.6 EXTRA MORTALITY Extra mortality attributable to NI is reported between 4% and 33%.12,18-20 The highest mortality rates are seen during nosocomial pneumonias.9 In a recent study in Argentina attributable deaths for urinary tract infections, catheter-related bloodstream infections and ventilator associated pneumonia is found as 5%, 25% and 35% respectively.19 INFECTION CONTROL PROGRAMMES Much is already being done to minimize the risk of acquiring an infection in hospital. Infection control programmes are the mainstay of all activities in decreasing the prevalence of NI. Infection control is the responsibility of all health care professionals, including managers and infection control standards have been developed as part of a controls assurance programme. An effective infection control programme would benefit patients and their careers, and release considerable health care resources for alternative use.21 Cost-effectiveness method is the most frequently used type of methods in infection control programs, besides cost-benefit, cost-minimization, cost-utility methods are used.22-24 Targets of studies on cost-effectiveness in NI control are; A. Surgical site infections, pneumonia and bloodstream infections are the most costly infections. It is suggested infection control measurements has a cost of approximately 1-6% of the total costs. Approximately one third of these infections are preventable merely by fully implementing the current infection control guideline recommendations. Antibiotics are some of the most expensive drugs used in hospitals consuming up to 30% of the total drugs budget. It is impossible to reduce costs without control of antibiotic usage, and infection control programmes without antibiotic control will be incomplete.25 From the detailed epidemiologic information obtained by using the NNIS methods, interventions were designed and implemented that have reduced specific NI rates. In a study in Brazilian hospitals using NNIS system the surgical site infection rate after cesarean section was reduced from 11.6% in 1993 to 5.9% in 1996 (p<0.05). Cost savings from a program to optimize the use of antimicrobial agents in one hospital was more than $1.8 million over a 45-month period.26 In a study by Haley et al. with the help of SENIC (Study on the Efficacy of Nosocomial Infection Control) Project and NNIS (National Nosocomial Infections Surveillance) they reduced their hospitals' infection by 32% with intensive infection surveillance and control programs and they maintain that nearly one-third of all NI could be prevented if all hospitals adopt the most effective programs.27 A systematic review to describe multi-modal intervention studies, as well as studies assessing exogenous cross-infection published during the last decade, in order to give crude estimate of the proportion of potentially preventable NI is performed. The evaluation of thirty reports suggests that great potential exist to decrease NI rates, from a minimum 10% to a maximum effect of 70%, depending on the setting, study design, baseline infection rates and type of infection.28 The results of a study in England suggest that, if the incidence of NI observed could be reduced nationally 10%, resources to the value of £ 93.1 million might be released. This would be equivalent-for example, to 364 056 bed days or 47 902 finished consultant episodes. These estimates may be considered the gross benefits of prevention which needs to be established by further studies.21 The Epic project is now developing national evidence-based guidelines for preventing healthcare associated infections.29 Economic modeling strategies evaluating potential cost savings from effective infection-control measures also reveal important data which is very useful for the hospitals.30,31 High mortality rates and economic expense which NI represents emphasizes the justification for measures of control of this entity. To estimate better the current personnel and financial resources necessary to support infection control activities and to prevent NI, it is imperative that those conducting studies of hospital epidemiology and healthcare outcomes research determine these current costs. REFERENCES
Copyright 2003 - Indian Journal of Medical Sciences. The following images related to this document are available:Photo images[ms03030t3.jpg] [ms03030t1.jpg] [ms03030t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}