 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
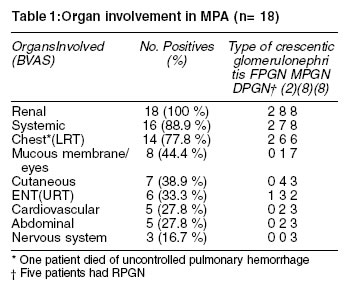
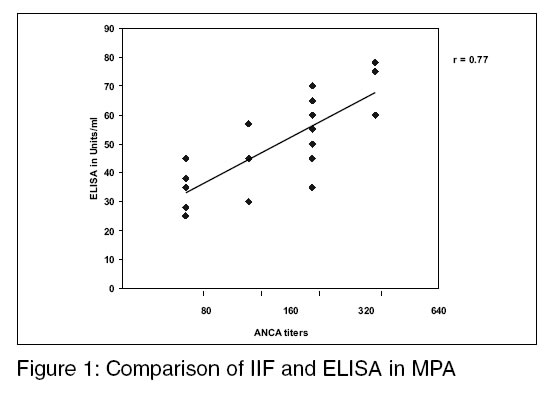
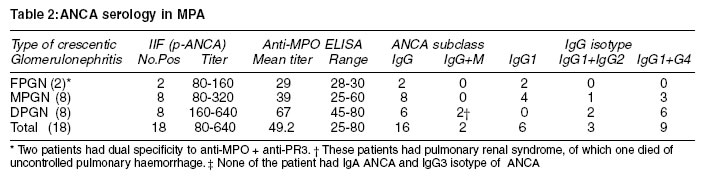
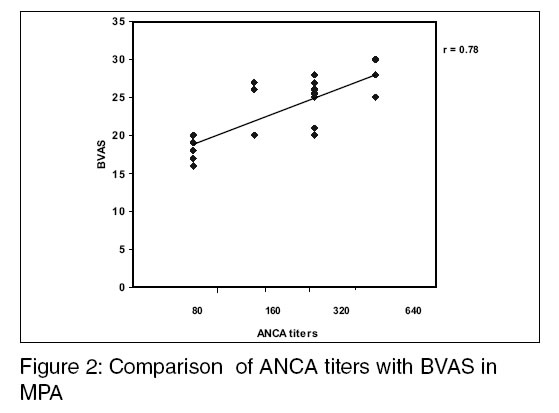
Indian Journal of Medical Sciences, Volume 57, Number 11, November 2003, pp. 479-486 Anti-Myeloperoxidase antibodies in patients with Microscopic polyangiitis V D Pradhan, S S Badakere, A R Pawar, A F Almeida* Department of Autoimmune Disorders, Institute of Immunohaematology, Indian Council of Medical Research, 13th Floor, K. E. M. Hospital, Mumbai 400012 and *Professor and Head, Department of Nephrology, K. E. M. Hospital, Mumbai-400012. Correspondence: Dr. S. S. Badakere, Deputy Director (S.G.), Institute of Immunohaematology, Indian Council of Medical Research, 13th Floor, K. E. M. Hospital, Mumbai-400012, India. E-mail: badakeresuresh@rediffmail.com Accepted Date: 29-10-2003 Code Number: ms03035 ABSTRACT Background & objectives: Anti-neutrophil cytoplasmic antibodies in active necrotizing and crescentic glomerulonephritis are associated with systemic vasculitides like Wegener's granulomatosis, Microscopic polyangitiis and Churg Strauss Syndrome. This study shows the incidence of ANCA with specificities to Myeloperoxidase and Proteinase3 in MPA cases and gives the correlation of ANCA with Birmingham Vasculitis Activity Score. KEY WORDS: Anti-neutrophil cytoplasmic antibodies, Microscopic polyangitiis, Indirect Immunofluorescence, Enzyme Linked Immunosorbent Assay, perinuclear-ANCA, Anti-Myeloperoxidase. Anti-neutrophil cytoplasm antibodies (ANCA) are directed against various components of neutrophil cytoplasm granules, and were first identified in patients with necrotizing glomerulonephritis.1 ANCA is now a specific and sensitive serological marker for active Wegener's granulomatosis (WG) and is also found to be useful in diagnosis of Microscopic polyangiitis (MPA), Churg Strauss Syndrome (CSS) and pauci-immune necrotizing crescentic glomerulonephritis (NCGN).2 Microscopic polyangiitis (MPA) was first described by Davson et al in 1948,3 in a subgroup of patients with polyarteritis nodosa (PAN) with segmental necrotizing glomerulonephritis and before the discovery of standardized ANCA detection methods, MPA was grouped with PAN and it was Zeek in early 1950's who named it as `Microscopic Polyangiitis' to reflect the actual clinical involvement in the disease.4 The presence of ANCA and few or no immune deposits in the involved vessels characterize this syndrome.5 The clinical features of MPA as summarized by some earlier workers have shown that in classical MPA syndromes there is a male preponderance in the age group of 40-60 years.6-9 The onset of illness is characterized by systemic involvement like fever, malaise, arthralgias, anorexia and weight loss in about 60 to 75% of the patients at the time of diagnosis. Renal involvement is the major feature and is characterized by `pauci-immune' or crescentic glomerulonephritis, which manifests as proteinuria, hematuria, and renal failure. About 50% of MPA cases may have pulmonary involvement where pulmonary haemorrhage has also been reported in about 12-30% of patients, being the main cause of morbidity and mortality.10 Upper respiratory tract involvement is less common in MPA as compared to WG and CSS and is seen in about 35 % cases, peripheral neuropathy especially motor mononeuritis multiplex. Musculoskeletal involvement such as myalgia, arthralgia and rarely arthritis occurs in about 65-72% of MPA patients where as ischemic ulceration of gut that causes pain in the abdomen and blood in the stool, bowel perforation and acute pancreatitis are rare but serious complications in MPA.11 In cases of MPA, the major target antigen of ANCA is Myeloperoxidase (MPO).12 ANCA can be detected in patient's serum by the immunofluorescence technique which is considered as a `gold standard' for ANCA detection13,14 however the more specific solid phase binding ELISA, using purified MPO, further adds to the specificity and quantitation of these autoantibodies.15 The main objectives of this study was to investigate the immunofluorescence patterns like perinuclear or cytoplasmic ANCA and their specificities to MPO and PR3 by ELISA in MPA cases, where the clinical severity was assessed by Birmingham Vasculitis Activity Score (BVAS). The renal manifestations seen in these cases were subdivided into focal proliferative glomerulonephritis (FPGN), membrano proliferative glomerulonephritis (MPGN) and diffuse proliferative glomerulonephritis (DPGN) and correlated with the serological and immunological findings. MATERIALS & METHODS In this study eighteen cases of MPA were investigated which were diagnosed as per the Chapel Hill Consensus Criteria (CHCC),5 while the classification of these cases was based on the American College of Rheumatologists (ACR) criteria.16 They were histologically proven crescentic and/or necrotizing glomerulonephritis with few or no immune deposits which were further grouped into FPGN, MPGN and DPGN but with no respiratory symptoms compatible with WG. Also BVAS was used to assess disease severity in these cases.17 This prospective study was carried out after obtaining the requisite Ethics Committee permission. Five ml of clotted blood was asceptically collected from patients referred by clinicians and the separated serum was stored at -200C. All these sera were HIV and HBsAg negative and relevant clinical, histopathological and laboratory data were appropriately recorded. Confirmation of the diagnosis of renal vasculitis necessitated renal biopsies examined by light microscopy which was done by staining slides with hematoxalin, eosin and periodic acid Schiff (PAS) staining. Immunofluorescence microscopy was done using anti-IgG, anti-IgM, anti-IgA, anti-C3, anti-C4 and anti-fibrinogen FITC conjugates on renal tissue collected in 10% buffered formalin from paraffin embedded blocks. ANCA were detected using human neutrophils (PMN) by IIF technique.18 Briefly, the method is as follows. PMN were used to prepare a cytospin substrate using Hettich Universal 16A cytocentrifuge and some slides were fixed with 96% ethanol and others with formalin. After reacting with patient's sera at 1: 20 dilution, the slides were probed using FITC tagged polyvalent anti-human globulin serum and observed under a fluorescent microscope, Nikon, Optiphot II, Japan. Microphotography was also done using an automated photography system, Nikon AFX II A, Japan. The slides were also examined using a Confocal Laser Scanning microscope. (LSM 510, Carl Zeiss, Germany) to visualize the patterns of immunofluorescence. The specificity of the antibodies were also identified by antigen binding ELISAs for anti-Myeloperoxidase (MPO) and anti-Proteinase3 (PR3) using kits from Genesis (UK). A value <3.0 u/ml was negative, 3-5 u/ml were equivocal and >5 u/ml were considered as positive. ELISAs for anti-MPO subclass and IgG isotype detection of anti-MPO was performed as per the method described by Locke et al, 1999.19 ANA was qualitatively and quantitatively tested by IIF test at a 1:20 dilution of test serum, using HEp-2 cells obtained from Enterovirus Research Center, ICMR, Mumbai which were maintained in a continuous culture and harvested at log phase of growth. The results were interpreted in terms of titers i.e. test sera showing immunofluorescence at its highest dilution.20,21 RESULTS Eighteen clinically and histopathologically diagnosed MPA cases were studied. The male to female ratio was 1.6:1 and the age range was 13 to 62 years with a mean + SD value of 34.6 + 13.5 years. All patients had active disease where the BVAS ranged from 17 to 30 with mean + SD value of 23 + 4. Also all had renal involvement where histopathology revealed crescentic glomerulonephritis. They were further grouped as 2 cases of FPGN, MPGN 8 cases and DPGN 8 cases. Also systemic involvement was seen in 88.9% with pulmonary involvement (LRT) in 77.8% cases where as upper respiratory tract involvement (URT) was seen in only 33.3% cases. Cutaneous involvement was seen in 38.9% cases and mucous membrane/eye involvement was seen in 44.4% cases. Cardiovascular and abdominal manifestations were present in 27. 8% cases each, and CNS involvement was seen 16.7% cases (Table 1). ANCA serology showed that all these patients had p-ANCA immunofluorescence pattern by IIF with titers ranging from 80-640, which were also detected by ELISA showing specificity to anti-MPO. Also, a good correlation was observed between IIF titers and ELISA values which were statistically significant. (r=0.77) (Figure 1). The IIF results seen on immunofluorescence microscopy were further scanned using a Confocal Laser Scanning microscope for the clarity of immunofluore-scence patterns. The break up of ANCA in a spectrum of crescentic glomerulonephritis in MPA is as shown in Table 2. All cases had anti-MPO antibodies but two cases of FPGN also had anti-PR3 as an additional antibody, and by ELISA showed the presence of anti-MPO and anti-PR3 in the same sera which could be detected only by respective ELISAs. These two cases had the pulmonary renal involvement with upper and lower respiratory tract involvement along with some systemic manifestations. ANCA immunoglobulin subclass studies showed the presence of IgG ANCA in 16/18 (88.7%) cases where as 2/18 cases (11.1%) had IgG+IgM ANCA. These two patients who had rapidly progressive glomerulonephritis (RPGN) had severe pulmonary renal manifestations, of which one patient died of uncontrolled pulmonary hemorrhage. Further ANCA IgG isotype studies showed that, the patients had IgG1 along with IgG4 in 9/18 cases (50%) and IgG2 in 3/18 cases (16.7%) and IgG3 isotype was absent in these patients. A good correlation was also observed with ANCA titers and BVAS in MPA cases (Figure 2). ANA was found to be present in 5/18 (27.8%) MPA cases. These cases were not granulocyte specific ANA (GS-ANA) as is sometimes seen in ANCA associated disorders. The differences between GS-ANA and ordinary ANA is that, the GS-ANA antibodies bind only to the nuclear components of granulocytes and do not react with nuclear components of other cell substrates used for ANA detection like HEp-2 cells, rat, liver or kidney sections etc. Perinuclear or p-ANCA shows a cytoplasmic immunofluorescence rim pattern just around and outside the nucleus of the PMN while ANA shows immunofluorescence of the nuclear components inside the nucleus. Both ANCA and ANA immunofluorescence patterns were screened using IIF microscopy and also further confirmed by Confocal Laser Scanning microscopy, while specificity of ANCA was identified by ELISA. DISCUSSION Vasculitis is known to be an important treatable cause of renal impairment that could lead to episodes of morbidity and mortality. It is characterized by inflammatory cell infiltration leading to necrosis of blood vessels.12 In an earlier five year Indian study11 six MPA patients were studied, with varied clinical spectra, and 50% of them presented as pulmonary renal syndrome. Also in most of the earlier studies6-9 a male preponderance in MPA has been reported, which is similar to the observations in the present study showing male to female ratio of 1.6:1. The use of BVAS which considers nine clinical parameters for estimating disease severity and also using ANCA titers for the clinical and serological assessment of vasculitis has greatly helped the clinicians to study this potentially life threatening disease where an early diagnosis and treatment could be life saving. The BVAS of patients in this study ranged from 17 to 30 score values but was found to be high in DPGN cases, though all patients had crescentic glomerulonephritis at presentation. Pulmonary renal manifestations were seen 77.8% of the cases as compared to URT with renal manifestations which were observed in 33% cases. Renal involvement, along with upper and lower respiratory tract is often a criteria for diagnosis of classical cases of WG,22 however it is differentiated from MPA by the presence of cytoplasmic ANCA (c-ANCA) immunofluorescence patterns and anti-PR3 antibodies detected by ELISA along with granuloma formation in the lungs. In MPA cases however no granulomatous lesions are seen in lungs and also there is absence of c-ANCA but the presence of p-ANCA along with anti-MPO antibodies is seen.23 This is a special immunodiagnostic point which is highly specific and may be used to differentiate these disorders, though very rarely p-ANCA in low titers have been observed in cases of WG.24 All patients showed p-ANCA pattern by immunofluorescence and Confocal microscopy along with anti-MPO antibodies, while only two patients in the FPGN group showed the rare dual specificity of both anti-MPO and anti-PR3 antibodies where the predominant ANCA was p-ANCA with high titers of anti-MPO while c-ANCA and anti-PR3 were comparatively in low titers showing dual specificity. Though IgG ANCA was predominantly seen among the patients, more severe clinical manifestations were seen in the two cases of DPGN along with pulmonary involvement having IgM+ IgG ANCA, having a BVAS of 27 and 25 respectively, out of which one patient died due to uncontrolled pulmonary haemorrhage. Both the cases had high titers of p-ANCA, and high ELISA values showing anti-MPO specificity. Jayne et al, 1991 and Kokolina et al, 1994 earlier had also reported excessive pulmonary haemorrhage in patients who had IgM ANCA and also ANCA isotype distribution could be related to clinical disease expression.25,26 IgG isotypes also showed quite interesting findings among these patients as they are known to differ in their biological implications. It is reported that all anti-MPO positive patients having IgG1 and IgG4 subclass could be related to recurrent exposition of the antigens, probably as a part of a hypersensitivity reaction. Also IgG4 is mainly produced after recurrent stimulation with antigen, which may suggest a chronic antigenic stimulation of B cells leading to ANCA.27 IgG4 was commonly seen in DPGN and MPGN probably indicating repeated antigenic exposure leading to stronger expression of disease. We have also encountered 27.8% cases of ANCA who were also having ANA, during immunofluorescence testing. In such cases, the IIF ANCA patterns become difficult to identify because of a strong nuclear fluorescence,28 but this problem can be solved by taking the ELISA results and if available the Confocal Laser Scanning microscopy for determining the true positivity and individual specificities to ANCA.29 In an international meeting of ANCA investigators held in 1996, to develop and standardize assays for the detection of ANCA, showed that all patients should be tested by IIF and if positive to be confirmed by ELISA.24 In conclusion, both the IIF test which is an ANCA screening assay, along with the Confocal Laser Scanning microscopy, and ELISA for determining specificity, need to be carried out to identify true positives and to detect the rare cases of ANCA showing dual specificities. The p-ANCA immuno-fluorescence pattern along with antibodies to MPO is highly diagnostic for MPA, and could be a useful diagnostic tool. A triad of investigations such as clinical findings as represented by BVAS, histopathological investigations, and ANCA patterns, titers and specificities, would surely go a long way in early diagnosis, patient care, initiation of treatment and survival. ACKNOWLEDGEMENTS We are grateful to the Indian Council of Medical Research (ICMR), Director, Institute of Immunohaematology for facilities provided to us to carry out this work and to Director, Entero Virus Research Centre for the HEp-2 cells used in this study. REFERENCES 1. Davies DJ, Moran JE, Niall JF, Ryan GB. Segmental glomerulonephritis with anti- neutrophil antibody: Possible arbovirus aetiology? Br Med J 1982;285:606-10. 2. Lhote F, Guillevin L. Polyarteritis nodosa, Microscopic polyangitiis and Churg Strauss Syndrome. Rheum Dis Clin North Am 1995;21:911-47. 3. Davson J, Ball J, Platt R. The kidney in periarteris nodosa. QJM 1948;17:175-202. 4. Zeek PM. Polyarteritis nodosa and other forms of necrotizing angiitis. N Engl J Med 1953;248:764-72. 5. Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL, et al, Nomenclature of systemic vasculitides: Proposal of an international consensus conference. Arthritis Rheum 1994;37:187-92. 6. Serra A, Cameron JS, Turner DR. Vasculitis affecting the kidney: presentation, histopathology and long term prognosis. Q J Med 1984;53:181-207. 7. Savage COS, Winearls CG, Evans DJ. Microscopic polyarteritis: presentation, pathology and prognosis. Q J Med 1987;56:467-74. 8. Agati DV, Chander PM. Idiopathic Microscopic polyarteritis nodosa: Ultrastructural observations on the renal vascular and glomerular lesions. Am J Kidney Dis 1986;9:95-8. 9. Adu D, Howie AJ, Scott DG, Bacon PA, Mc Gonigle RJ, Micheal J. Polyarteritis and the kidney. Q J Med 1987;62:221-37. 10. Savige J, Davies D, Falk RJ, Charles Jennette J, Wiik A. Anti-neutrophil cytoplasmic antibodies and associated diseases: A review of the clinical and laboratory features. Kidney International 2000;57:846-62. 11. Handa R, Wali JP, Gupta SD, Dinda AK, Aggrwal P, Wig N, Biswas A. Classical Polyarteritis Nodosa and Microscopic Polyangiitis- A Clinicolpathologic Study. JAPI J Assoc Physicians India 2001;49:314-9. 12. Csernok Elena, Muller A, Goss WL. Immunopathology of ANCA-associated vasculitis. Int Med 1999;38:759-65. 13. Badakere SS, Pradhan VD. ANCA: Anti-neutrophil cytoplasmic antibodies and their role in vasculitis associated kidney disorders. Ind J Med Sci 2002;56:335-9. 14. Hagen EC, Andrassy K, Csernok E, Daha MR, Gaskin G, Gross W, et al, The value of indirect immunofluorescence and solid phase techniques for ANCA detection: A report on the 1st phase of an international cooperative study on the standardization of ANCA assays. J Immunol Methods 1993;159:1-16. 15. Savige J, Gills D, Benson E, Davis D, Esnault V, Falk RJ. et al. International consensus Statement on Testing and Reporting of Anti-neutrophil Cytoplasmic Antibodies (ANCA). Am J Clin Pathol 1999;111:507-13. 16. Luqmani RA, Bacon PA, Moots RJ, Janssen BA, Pall A, Emery P, et al. Birmingham Vasculitis Activity Score (BVAS) in systemic necrotizing vasculitis. Q J Med 1994;87:671-8. 17. Hunder G. Vasculitis: Diagnosis and therapy. Am J Med 1996;100:37S-45S. 18. Rasmussen N, Sjolin C, Isaksson B, Bygren P. and Wieslander J. An ELISA for the detection of anti-neutrophil cytoplasm antibodies (ANCA). J Immunol Methods 1990;127:139-45. 19. Locke C, Leaker B, Camnridge G. A comparison of the characteristic of circulating anti-myeloperoxidase autoantibodies in vasculitis with those in non-vasculitic conditions. Clin Exp Immunol 1999;115:369-76. 20. Badakere SS, Chablani AT, Bhatia H. Anti-nuclear factor in some autoimmune disorders. Proc. Recent Trends in Immunohaematol. IIH, ICMR 1982;101-8. 21. Badakere SS, Chablani AT. Immunofluorescent techniques in immunohaematology. Immunohaemat. Bull 1985;16:1-4. 22. Gross WL, Schmitt WH, Csernok E. ANCA and associated diseases: Immunodiagnostic and pathogenetic aspects. Clin Exp Immunol 1993;91:1-12. 23. Pradhan VD, Badakere SS, Iyer YS, Kumar R, Almeida AF. A study of anti-neutrophil cytoplasm antibodies in systemic vasculitis and other related disorders. J Postgrad Med 2003;49:5-10. 24. Hagen EC, Daha M, Hermans J, Andrassy K, Csernok E , Gaskin G, et al. Diagnostic value of standardized assays for anti-neutrophil cytoplasmic antibodies in idiopathic systemic vasculitis. Kidney International 1998;53:743-53. 25. Jayne DRW, Weetman AP, Lockwood CM. IgG subclass distribution of autoantibodies to neutrophil cytoplasmic antigens in systemic vasculitis. Clin Exp Immunol 1991;84:476-81. 26. Kokolina E, Noel L, Nusbaum P, Geffriaud C, Grunfeld J, Halbwachs-Mecarelli L, et al. Isotype and affinity of anti-myeloperoxidase autoantibodies in systemic vasculitis. Kidney International 1994;46:177-84. 27. Brouwer E, Cohen Tervaert JW, Horst G, Huitema MG, van der Giessen M, Limburg C, et al. Predominance of IgG1 and IgG4 subclass of anti-neutrophil cytoplasmic autoantibodies (ANCA) in patients with Wegener's granulomatosis and clinically related disorders. Clin Exp Imunol 1991;83:379-86. 28. Bang Ia Cour B, Wiik A, Hoier-Madson M, Baslund B. Clinical correlates and substrate specificities of antibodies exhibiting neutrophil nuclear reactivity- a methodological study. J Immunol Methods 1995;187:287-95. 29. Skogh T, Dahlgren C, Holmgren K, Peen E. and Stendahl O. Anti-granulocyte antibodies (cANCA, p-ANCA, GS-ANA) studied by Confocal Scanning Laser fluorescence microscopy, ELISA and chemiluminescence techniques. Scan J Immunol 1991;34:137-45. Copyright 2003 - Indian Journal of Medical Sciences. The following images related to this document are available:Photo images[ms03035t2.jpg] [ms03035t1.jpg] [ms03035f1.jpg] [ms03035f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}