 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
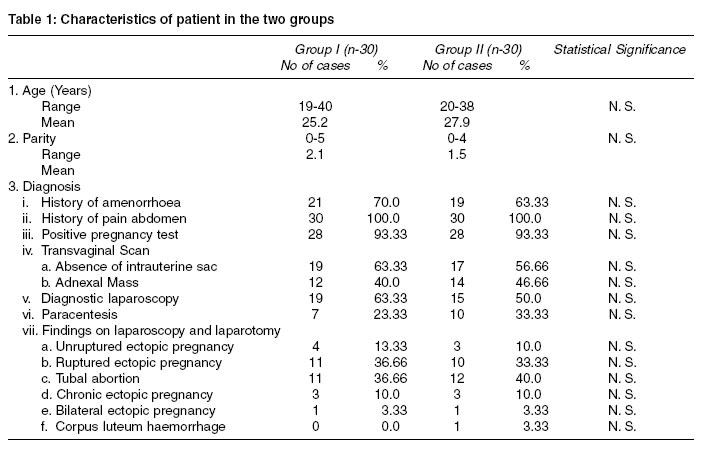
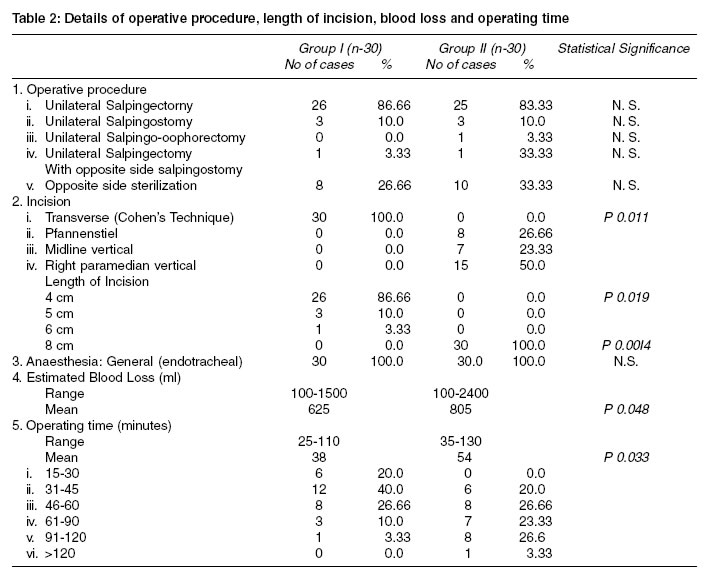
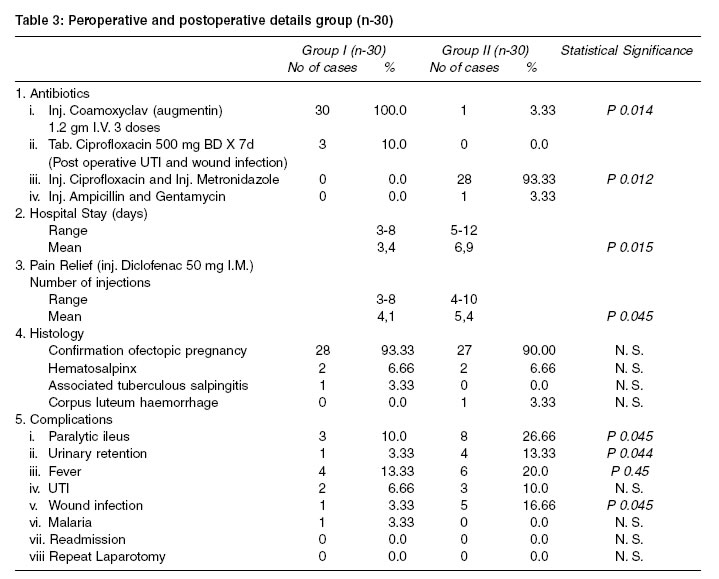
Indian Journal of Medical Sciences, Volume 57, Number 11, November 2003, pp. 493-500 A randomized controlled comparison of minialpartomy and lapartomy in ectopic pregnancy cases J B Sharma, S Gupta,* M Malhotra,** R Arora*** MD, MRCOG, Associate Professor; *MD, Assistant Professor; **MD, Senior Research Associate; ***MD, Professor; Department of Obstetrics and Gynaecology, Maulana Azad Medical College and associated Lok Nayak Hospital New Delhi-110002, India. Correspondence: Dr. J. B. Sharma, AI/61, Azad Apartments, Accepted Date: 21-11-2003 Code Number: ms03037 ABSTRACT Backround: As ectopic pregnancy is associated with significant maternal mortality and morbidity it maybe worthwhile to find alternative surgical method to traditional laparotomy. Key Words: Minilaparotomy, Laparotomy, Surgery, Ectopic pregnancy. INTRODUCTION Laparotomy has been the traditional method of treating gynecological pelvic pathology. The advantages of open surgery include manual contact with pelvic anatomy and easy access allowing blunt dissection with fingers as an adjunct to the sharp and scissors dissection.1 Laparoscopic surgery has become popular especially in unruptured ectopic pregnancy cases as it reduces the potential for trauma and morbidity associated with laparotomy with minimum postoperative morbidity.2 But laparoscopy has been limited in its general acceptance by the extra cost of disposable equipment, increased operative time, dedication of instruments and training of surgeons in new and unfamiliar skills.3 Things are worse in third world countries where such expensive instruments are not available in most of the hospitals.4 Laparoscopic surgery for ectopic pregnancy is routinely performed in most developed countries as it has the advantage of shorter hospital stay and is associated with less postoperative morbidity and less need of analgesics. The cost of laparoscopic surgery is high but can be significantly reduced by using instruments made in India especially the reusable ones. However, the expertise for operative laparoscopic surgery is still not available in India stressing the need for finding alternatives to the traditional laparotomy. Medical management for ectopic pregnancy is now an established treatment in some centers but can only be done in small sized unruptured ectopic pregnancies, in haemodynamically stable patients and in centres with facilities for serum beta hCG estimation. Unfortunately most patients in developing countries come very late with ruptured ectopic pregnancy and shock, where medical treatment cannot be performed. Minilaparotomy has been an established technique in gynaecology mainly for its use in sterilization operations.5-7 It has been successfully used by general surgeons for cholecystectomy, bowel surgery, prostatectomy and radical cystectomy where it competes very favorably with laparoscopic surgery.8-11 Minilaparotomy has recently been used in gynecological surgeries like ovarian cysts, reversal of sterilization and other benign gynecological diseases with very promising results. Two recent studies including one by the first author of this article have proven that minilaparotomy hysterectomy can be safely done in selected patients.4,15 Combined laproscopy, minilaprotomy hysterectomy and minilaparotomy assisted vaginal hysterectomy have been described in the literature.16,17 The present study was conducted to see the feasibility, costeffectiveness and safety of minilaparotomy for ectopic pregnancy cases as compared to traditional laparotomy. MATERIAL AND METHODS A total of 60 patients for suspected ectopic pregnancy were included in the study over a period of three years.Patients with significant medical disease like diabetes, hypertension and previous laparotomy were excluded from the study in both the groups.The women who were not willing to participate were excluded from the study. The patients were randomly divided into two groups using computer generated numbers. Group I (30 cases) were managed by minilaparotomy technique while other 30 patients (Group II) were operated by standard laparotomy technique. The choice of type and length of incision in group II was left to the operating surgeon. Ethical clearance to conduct the study was taken from local review board of the hospital. Informed written consent was taken from all the patients informing them that they could be randomized to either of the groups. Laparoscopy was performed to confirm the diagnosis of ectopic pregnancy in 19 (63.33%) cases in-group I and 15 (50%) cases in group II. Paracentesis confirmed haemoperitoneum in 7(23.33%) cases in-group I and in 10 (33.33%) cases in group II. Four patients (13.33%) in group I and 5 patients (16.66%) in-group II were straightaway taken up for minilaparotomy or laparotomy as they were in shock. Group I patients were operated by minilaparotomy technique in which the skin was incised by 4-6 cms long suprapubic transverse incision and the abdomen was opened by Cohen's technique (tearing rectus sheath laterally with fingers and opening the peritoneum with fingers). The fundus of the uterus was exteriorized using two fingers of right hand along with the affected fallopian tube. No packs or retractors were used. The tube was held with the Babcock clamp. Depending on the age and parity of the patient, condition of the effected tube and opposite fallopian tube, either salpingectomy or salpingostomy was performed. Salpingectomy was preferred where family was complete or tube was ruptured. The tube was sent for histopathological examination in all the cases. The peritoneal cavity was cleared of all the blood and blood clots using repeated saline irrigation. Complete haemostasis was achieved. Both ovaries, uterus and opposite side fallopian tube were examined for normality. Sterilization in the opposite tube was performed by Pomeroy's technique if the patient demanded it and had completed her family. Abdomen was closed using No. 1-0 polyglycolic suture to rectus sheath and continuing the same suture as subcuticular skin suture. Peritoneun was not closed. All patients received three doses of 1.2 gm intravenous coamoxyclav at 8 hourly intervals. The other 30 patients were operated by standard laparotomy procedure (more than 6 cms incision) by vertical or pfannenstiel incision, with insertion of abdominal packs and retractors. The surgical procedure done was as per requirement (salpingectomy or salpingostomy). The antibiotics given were ciprofloxacin and metronidazole for seven days. Blood transfusion was given if required. Patients with postoperative fever, UTI or wound infection were given alternative antibiotic depending upon the culture sensitivity. Postoperatively patients were given 2 litres of intravenous fluids on the day of surgery. Injection diclofenac sodium 50 mg intramuscularly was given whenever necessary upto a maximum of 3 injections in 24 hours. Oral clear fluids were started when bowel sounds were heard. Semisolid diet was started from the second day and normal diet from 3rd day onwards provided bowel sounds were heard. They were mobile from 6 hours onwards, if they felt well. Patients were discharged if there were no complications and were seen in the outpatient clinic after 2 weeks for any complications and to collect their histopathology report. Results were compiled and statistical analysis was performed. Chi square test was used and a P value of <0.05 was used as level of significance. RESULTS A total of 60 patients of ectopic pregnancy who were operated by minilaparotomy (30 cases) or laparotomy (30 cases) were studied. The characteristics of the patients (age and parity) are shown in Table 1. The conversion from minilaparotomy to laparotomy was not required in any of the cases allocated to group I. All patients were given general anaesthesia.The operative details of the patients are depicted in Table 2. The mean blood loss was 625 ml and 805 ml respectively in the two groups and was mainly due to basic pathology rather than the surgical procedure. There was no significant difference in the requirement of blood transfusion in the 2 groups as it was given in 20 cases (66.6%) in group I and 21 cases (70%) in group II. Mean operative time taken was 38 minutes in group I and 54 minutes in group II which was statistically significant (P<0.05) (Table 2). The less time taken was due to Cohen's technique which is very fast, avoidance of use of packs and retraction and avoidance of closure of peritoneum and muscles in minilaparotomy technique. Peroperative and post operative details are shown in Table 3. The complications are shown in Table 3. Paralytic ileus was seen in 3 (10%) cases in group I and all of these were patients with chronic etopic pregnancy where gut was adherent to the tube. The incidence of paralytic ileus was much higher in group II, that is, 8 cases (26.66%) (P<0.05). No patient required readmission or relaparotomy. Mean hours of mobility, starting normal diet and discharge from hospital were 10 and 24 hours, 1.5 days and 3.1 days and 3.4 days and 6.9 days respectively in the two groups which was statistically significant (P<0.05). Histological findings are shown in Table 3. DISCUSSION The present study clearly demonstrates that minilaparotomy can be used safely and costeffectively as an alternative to traditional laparotomy for the management of ectopic pregnancy cases. Ectopic pregnancy is conventionally managed by laparotomy and salpingectomy where patient has to stay in hospital for many days and there are more complications and slow recovery. Laparoscopy is becoming treatment of choice in selected patients but needs expensive equipment, intense training and may not be suitable for all cases and is limited in its scope in developing countries. Our hospital has facilities only for diagnostic laparoscopy and laparoscopic sterilization but not for laparoscopic surgery. Medical management with parenteral administration of methotrexate or local instillation of chemicals is practised in some hospitals but is suitable for very selected haemodynamically stable and unruptured small ectopic pregnancy cases with, facilities for monitoring of serum beta hCG levels, so it cannot be used routinely especially in third world countries. Minilapaortomy is an attractive option especially in third world countries as it does not require expensive equipment as routine instruments are used and can be learnt easily by all surgeons. The beauty of the technique is that in case it is not feasible to do the procedure through minilaparotomy, the incision can be extended on either side without changing the position. The patients do very well and there are minimum postoperative complications. As no packs or retractors are used, so there is minimum gut or bladder handling with least complications. Minilaparotomy has been successfully used in surgical procedures,8-11 sterilisation operation,5-7 gynaecological disorders like recanalization operations and ovarian cysts12-14 and minilaparotomy hysterectomy1,15 with excellent results. Endoscopic minilaprotomy hysterectomy and minilaparotomy assisted vaginal hysterectomy have also been reported in the literature.1,16,17 The results of the present study are quite good and better than laparotomy. There are minimum post operative complications, early ambulation and start of normal diet, early recovery, discharge and return to work without the need of expensive instruments and strenuous training. Complications like paralytic ileus, urinary retention and wound sepsis were less common in minilapartomy technique than in laparotomy. In group I all cases were operated by minilaparotomy technique using a small transverse incision. In group II the length and type of incision was left to the surgeon. This maybe a limiting factor in the present study as vertical long incision may itself cause higher postoperative morbidity. But this is precisely the message we want to convey to the the readers that small transverse incision is associated with better outcome than long vertical or transverse incision. As sterlisation operation was performed wherever indicated in the same sitting it can theoretically bias the results. However, the numbers of sterlisations were similar in the two groups not to cause any undue bias. Inclusion of body mass index would have better and might explain the length of abdominal incision. Unfortunately it was not taken into consideration in the present study. However, the patients were randomly allocated to the two groups and both the groups had obese patients. To conclude minilaparotomy appears to be a costeffective and safe alternative to standard laparotomy for the surgical management of ectopic pregnancy with the advantage of obiviating the need of expensine equipment and shorter learning curve. REFERENCES 1. Maher PJ, Wood EC, Hill DJ. Endoscopic minilaparotomy. Aust NZ J Obstet Gynaecol 1995;35:76-8. 2. Shaxted EJ. Minimal invasive endoscopic surgery for gynaecological emergencies. In Studd JJ, editor. Progress in Obstetrics and Gynaecology volume II. Churchill Livigstone Edinburgh 1994;273-280. 3. Robert ER, Mikolaos B, Adam LM. Is laparoscopic hysterectomy a waste of time? Lancet 1995;345:36-41. 4. Sharma JB. Minilaparotomy abdominal hysterectomy - A new surgical technique. Obs Gyn Commun 1999;1:28-31. 5. Cisse CT, Kerby K, Cisse ML, Diallo D, Moreira P, N'Dong I, et al. Tubal Ligation using minilaparotomy under local anaesthesia. Apropos of 800 cases at the University Hospital Centre in Dakar. Contraception Fertilite Sexualite 1997;25:10-15. 6. Taneepanichskul S, Intaraprasert S, Chaturachinda KI. Interval female sterillization of HIV-I positive women laparoscopy versus minilaparotomy. Int J Gynecol Obstet 1997;57:183-4. 7. Ruminjo JK, Lynam PF. A fifteen year review of female sterilization by minilaparotomy under local anaesthesia in Kenya. Contraception 1997;55:249-60. 8. Prudkov MI. Minilaparotomy and "open" laparoscopic surgeries in treatment of patients with cholelithiasis. Khirurgiia 1997;1:32-5. 9. Fursternberg S, Goldman S, Machado M, Jarhult J. Minilaparotomy approach to tumours of the right colon. Dis Col Rect 1998;41:997-9. 10. Lezin MS, Cherrie R, Cattolica EV. Comparison of laparoscopic and mainilaparotomy pelvic lymphadenectomy for prostate cancer staging in a community practice. Urology 1997;49:60-4. 11. Puppo P, Perachino M, Ricciotti G, Bozzo W, Gallucci M, Carmignani G. Laparoscopically assisted transvaginal radical cystectomy. Eur Urol 1995;27:80-4. 12. Flynn M, Niloff JM. Minilaparotomy for the ambulatory management of ovarian cysts. Am J Obstet Gynecol 1995;173:1727-30. 13. Slowey MJ, Coddington CC. Microsurgical tubal anastomosis performed as an outpatient procedure by minilaparotomy are less expensive and as safe as those performed as an inpatient procedure. Fertil Sterill 1998;69:492-5. 14. Benedetti-Panici P, Maneschi F, Cuttillo G, Scambia G, Cogiu M, Mancuso S. Surgery by minilaprotomy in benign gynaecological diseases. Obstet Gynecol 1996;87:456-9. 15. Hoffman MS, Lynch CM. Minilaparotomy hysterectomy. Am J Obstet Gynecol 1998;179:316-20. 16. Wood C, Maher P. Laparoscopic minilaparotomy hysterectomy. Aust NZ J Obstet Gynecol 1995;35:204-7. 17. Kohama T, Hashimoto S, Ueno H, Terada S, Inoue M. A technique of minilaparotomy assisted vaginal hysterectomy. Obstet Gynecol 1997;89:127-9. Copyright 2003 - Indian Journal of Medical Sciences. The following images related to this document are available:Photo images[ms03037t3.jpg] [ms03037t1.jpg] [ms03037t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}