 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
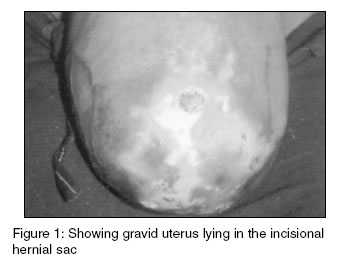
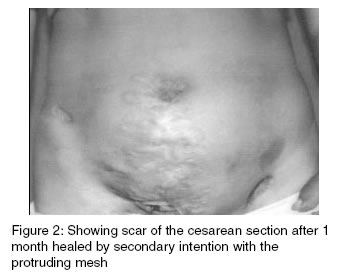
Indian Journal of Medical Sciences, Volume 57, Number 11, November 2003, pp. 501-503 Case report Successful pregnancy outcome after cesarean section in a case of gravid uterus growing in an incisional hernia of the anterior abdominal wall M Malhotra, J B Sharma,* L Wadhwa,** R Arora*** MD, Senior Research Associate; *MD, MRCOG, Associate Professor; **MD, DNB, Senior Resident; ***MD, Professor, Department of Obstetrics & Gynaecology, Maulana Azad Medical College & Associated, Lok Nayak Hospital, New Delhi-110002, India. Correspondence: Dr. J. B. Sharma, A 1/61, Azad Apartments, Sri Aurobindo Marg, New Delhi-110016, India. Accepted Date: 30-10-2003 Code Number: ms03038 ABSTRACT We herein report a case of a pregnant woman with previous cesarean section whose uterus herniated in an incisional hernia of the anterior abdominal wall at 34 weeks of pregnancy. Incarceration of the pregnant uterus in an incisional hernia is a rare but serious obstetric situation. Treatment is conservative till term followed by delivery and herniorrhaphy as was done in our case and it was associated with successful outcome. KEY WORDS: Pregnancy, Incisional hernia, Gravid uterus, Cesarean section. INTRODUCTION The presence of gravid uterus in an anterior abdominal wall incisional hernia is very rarely encountered in obstetric practice.1-4 It is a serious obstetric situation and may require emergency operative reduction. The management protocol depends upon the period of gestation. As pregnancy progresses the risk of incarceration increases and can lead to strangulation of uterus and subsequent complications. Conservative management is preferred till term in form of rest and abdominal binders. Herniorrhaphy is postponed until after the delivery.5 Here we report a case where the gravid uterus herniated through the anterior abdominal wall incisional hernia at 34 weeks gestation. An emergency cesarean section with removal of redundant skin was associated with a successful outcome although skin incision gaped and healed by secondary intention. CASE REPORT A 28-years-old Hindu Indian woman presented at 34 weeks of gestation of her third pregnancy with undue distention of the abdominal wall. She had a normal vaginal delivery 4 years back but had an emergency cesarean section two years back for acute fetal distress in a private hospital with vertical incision. There was history of infection in the cesarean wound for which antibiotics were given. On examination, she was moderately built and nourished. There was mild pallor. Pulse was 80 beats per minute and blood pressure was 112/78 mmHg. Heart and Chest were normal on auscultation. Abdominal examination revealed distention in the central area. Uterus was felt just underneath the skin with complete lack of anterior abdominal wall (Figure 1). The overlying skin showed ulcerations. Fetus was lying in the longitudinal lie with cephalic presentation in the herniated gravid uterus outside the abdominal cavity. Haemogram and urine examination were normal. Ultrasound showed the uterus herniated in the incisional hernia of the anterior abdominal wall. Live fetus with cephalic presentation with no gross congenital abnormalities and with placenta in the upper uterine segment was detected. She was kept admitted in the hospital on bed rest and abdominal support. Emollients and Neosporin skin ointment were applied over the skin of the anterior abdominal wall. Patient started to have labor pains at 37 weeks of pregnancy and an emergency section was performed and a female baby weighing 2.25 kg with APGAR of 7/10 at 1 minute and 9/10 at 5 minutes was extracted. The redundant abdominal wall was removed. There was no evidence of rectus sheath in the vicinity of the incision. Herniorrhaphy was performed with prolene mesh put anterior to rectus abdominis muscle and skin sutured. She was given a course of antibiotics. Unfortunately the skin wound gave way and the mesh protruded out. The skin wound healed by secondary intention in a month's time at home with regular antibiotic dressing from the hospital after discharge from the hospital on the 15th day. (Figure 2). She and the baby were doing well on a 6 weeks follow up visit and the wound had healed by secondary intention by then with a broad scar. DISCUSSION Cesarean section is the most commonly performed operation with overall rate being almost 25% in USA.1 Remote complications can be incisional hernia due to defective abdominal wound healing and herniation of the gravid uterus through the abdominal wall is a rare complication. The complications which have been reported in association with this condition include strangulation, abortion, premature labor, accidental haemorrhage, intrauterine death and rupture of the lower uterine segment.6 It interferes with proper growth and may cause intrauterine growth retardation Excessive stretching of the skin causes ulceration as in the present case due to friction between the hernia sac and other parts of the patients body. Cesarean section should be performed for successful outcome as in the present case. Herniorrhaphy can be performed during pregnancy if there is risk of morbid incarceration or skin is necrosed5 but can be postponed until delivery as the enlarged uterus may interfere with repair healing as was done in the present case. REFERENCES 1. Cesarean section. In: Cunningham FG, Gant NF, Levno KJ, Gilstrap LC, Hauth JC, Wenstrom KD, editors. Williams Obstetrics. 21st edn. Mc Graw Hill, New York; 2001. pp. 537-66. 2. Murphy KW. Reducing the complications of cesarean sections. In: Bonnar J, editor. Recent advances in Obstetrics and Gynaecology. Edinburgh: Churchill Livingstone; 1998. Vol 20. pp. 141-52. 3. Aimakhu VE. Gravid uterus in an anterior abdominal wall hernias. Int J Gynecol Obstet 1975;13:177-80. 4. FullMan PM. An incisional hernia containing an incarcerated twin pregnant uterus. Am J Obstet Gynecol 1971;111:308-9. 5. Deka D, Banerjee N, Takkar D. Incarcerated pregnant uterus in an incisional hernia. Int J Gynaecol Obstet 2000;70:377-9. 6. Dare FO, Makinde OO, Lalwal OO. Gravid uterus in an anterior abdominal wall hernia of a Nigerian woman Int J Gynaecol Obstet 1990;32: 377-9. Copyright 2003 - Indian Journal of Medical Sciences. The following images related to this document are available:Photo images[ms03038f1.jpg] [ms03038f2.jpg] |
| |||||||||

{kind=link}
{kind=link}