 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
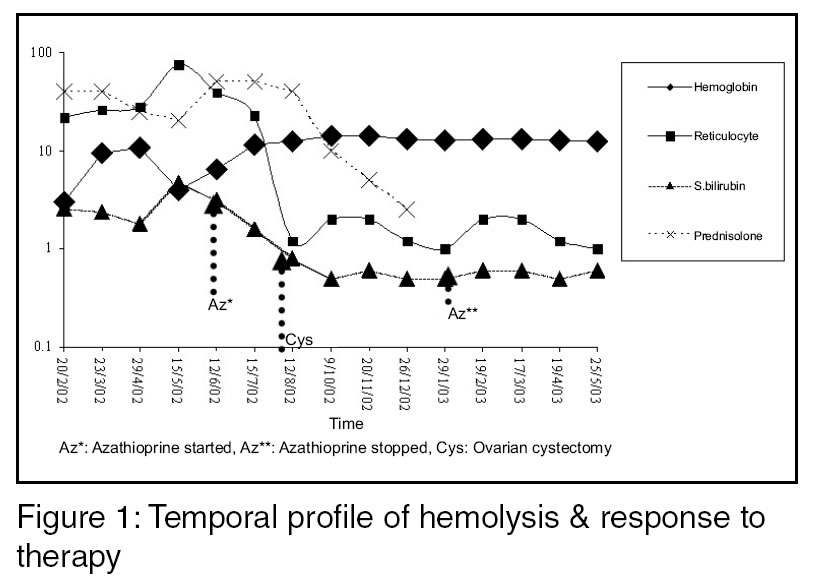
Indian Journal of Medical Sciences, Volume 57, Number 11, November 2003, pp. 504-506 Case report Autoimmune Hemolytic Anemia Associated With Benign Ovarian Cyst: A Case Report and Review of Literature V Agarwal, A Sachdev, R Singh,* S Lehl,* S Basu*,** DM, *MD; Departments of Medicine, **Hematology & Transfusion Medicine, Government Medical College & Hospital, Sector 32, Chandigarh, India. Correspondence: Dr Vikas Agarwal, Senior Lecturer, Department of Medicine, C1221, Sector 32B, Chandigarh, 160030, India. Accepted Date: 13-11-2003 Code Number: ms03039 ABSTRACT A 28-years-old female presented with severe autoimmune hemolytic anemia (AIHA), warm antibody mediated, and right side tubo-ovarian (TO) mass. There was sub-optimal response to immunosuppressive therapy (IST). Eight months later she underwent ovarian cystectomy which resulted in complete remission of AIHA without the need for IST. Pathological examination of the TO mass revealed benign ovarian cyst. Our case highlights the need to search for ovarian cyst/mass in females presenting with AIHA. Since immunosuppressive therapy is usually ineffectual in AIHA associated with ovarian cyst, it may be appropriate to contemplate surgery before embarking on IST in such cases. KEY WORDS: Ovarian cyst, Cystectomy. INTRODUCTION Autoimmune hemolytic anemia (AIHA) occurs as a primary disorder or secondary to lymphoproliferative syndromes, drugs, connective tissue diseases and infections. Rarely ovarian tumors have been reported to be associated with AIHA.1 Most of these tumors have been dermoid cysts. Herein we report one such rare cause of AIHA associated with benign ovarian cyst, with the aim of increasing awareness about this curable form of AIHA. CASE REPORT A 28-years-female presented with easy fatigability, pallor and amenorrhoea of 2 months duration and altered sensorium of 2 days duration. There was no history of jaundice, bone pains, bleeding, gall stones or peripheral neuropathy. Examination showed severe pallor, mild icterus, hepato-splenomegaly, and a haemic cardiac murmur. Rest of the general and systemic examination was unremarkable. Investigations revealed: hemoglobin 3 gm/dl, reticulocytosis 25%, anisocytosis, spherocytosis and polychromasia on peripheral smear, normal platelets, total and differential leukocyte counts, indirect hyperbilirubinemia with mildly deranged serum aspartate amino transferase. Direct and indirect Coomb's tests were positive (polyspecific sera against IgG and complement). Cold agglutinins were negative. Chest roentgenogram was normal. Ultrasonogram of the abdomen revealed right sided tubo-ovarian (TO) mass. Serological tests for antinuclear, anticardiolipin antibodies, HBsAg, anti HCV and anti HIV-1 and -2 were negative. She received 3 units of packed red blood cells followed by prednisolone 1mg/kg/day. Azathioprine was added after 4 months of inadequate response to glucocorticoids (Figure 1). Eight months after the diagnosis of AIHA, she underwent ovarian cystectomy, due to inadequate response to immunosuppressive therapy. Following ovarian cystectomy her hemolysis subsided without the need of immunosuppressive therapy within 4 weeks. Histopathological examination of the TO mass revealed benign ovarian cyst. Coomb's test six months later was negative. DISCUSSION The association between AIHA and ovarian tumors has been known since 1938,2 and complete resolution of hemolysis has been reported following removal of the tumor.1,3 The temporal association between cessation of hemolysis, negative Coomb's test and ovarian cystectomy in our case favors a strong possibility of association between the two. However, in view of prior use of glucocorticoids and azathioprine, a delayed response to these agents cannot be excluded. Our patient failed to respond to azathioprine and glucocorticoids and thus was a fit case for splenectomy. Since, ovarian cystectomy is known to cure AIHA in patients failing on splenectomy,1,3,5 we decided for removal of the ovarian cyst. Payne et al had reviewed the clinical course and response to ovarian cystectomy of 19 cases reported in the literature till 1981.3 Seven new cases since 1981, one described by Payne et al, and six others,6-11 (2 in Japanese and English, one each in Dutch and French languages) makes the total number of cases to twenty six till date. Of these twenty six cases, we were able to review the data for 20 cases. Seventeen cases, who had earlier failed on glucocorticoids or splenectomy, responded to ovarian cystectomy. One patient underwent ovarian cystectomy within 3 weeks of diagnosis but had shown a response to glucocorticoids as well.3 Two patients had died prior to surgery due to intestinal obstruction and transfusion reaction each. One patient had undergone ovarian cystectomy and splenectomy simultaneously followed by complete recovery. In this patient splenic sequestration of the labeled erythrocytes was documented postoperatively suggestive of negligible therapeutic effect of splenectomy. Time to resolution of hemolysis and disappearance of autoantibody following ovarian cystectomy has been reported to vary from 2 weeks to 7 months.3 In our patient hemolysis subsided within 4 weeks and autoantibodies disappeared after 6 months of ovarian cystectomy. Thus we conclude, though an association between AIHA and ovarian cyst is rare, its recognition is important as it presents an opportunity for definitive management and spares the need for potentially risky immunosuppressive therapy and splenectomy. References 1. Young RH, Scully RE. Sex cord-stromal, steroid cell and other ovarian tumors with endocrine, paraendocrine, and paraneoplastic manifestations. In: Kurman RJ, editor. Blaustein's Pathology of the Female Genital Tract. 5th edn. New York: Springer; 2002. pp. 906-66. 2. West-Watson WN, Young CJ. Failed splenectomy in acholuric jaundice and the relation of toxaemia to the hemolytic crisis. Br Med J 1938;1:1305-9. 3. Payne D, Muss HB, Homesley HD, Jobson VW, Baird FG. Autoimmune hemolytic anemia and ovarian dermoid cysts: case report and review of the literature. Cancer 1981;48:721-4. 4. De ruyere M, Sokal G, Devoitville JM, Fauchet D MCh, de spa V. Autoimmune hemolytic anemia and ovarian cyst. Br J Haematol 1971;20:83-94. 5. Barry KG, Crosby WH. Autoimmune hemolytic anemia arrested by removal of an ovarian teratoma : review of the literature and report of a case. Ann Intern Med 1957;47:1002-7. 6. Murad MD, Mohler DN, Carpenter JT Jr. Remission of immune hemolytic anemia after removal of ovarian dermoid cyst: case report. Va Med 1982;109:187-90. (Abstract) 7. Carreras Vescio LA, Toblli JE, Rey JA, Assaf ME, De Maria HE, Marletta J. Autoimmune hemolytic anemia associated with an ovarian neoplasm. Medicina B Aires 1983;43:415-24. (Abstract) 8. Wassenaar H, van der Meulen FW, Engelfriet CP, Kurstjens RM. Autoimmune hemolytic anemia caused by a dermoid cyst of the ovary. Ned Tijdschr Geneeskd 1984;128:113-7 (Abstract) 9. Ikeda K, Imazono Y, Shimamoto Y, Sato H, Kaneko S, Nishimura J, et al. A case of autoimmune hemolytic anemia associated with ovarian dermoid cyst. Rinsho Ketsueki 1985;26:212-6. (Abstract) 10. Suzuki H, Sugiki Y, Tanaka T, Hiroshi Y, Suzuki K, Otsu F, et al. A case of autoimmune hemolytic anemia following ovarian dermoid cyst. Nippon Naika Gakkai Zasshi 1993;82:1266-8. (Abstract) 11. Glorieux I, Chabbert V, Rubie H, Baunin C, Gaspard MH, Guitard J, et al. Autoimmune hemolytic anemia associated with a mature ovarian teratoma. Arch Pediatr 1998;5:41-4. (Abstract) Copyright 2003 - Indian Journal of Medical Sciences. The following images related to this document are available:Photo images[ms03039f1.jpg] |
| |||||||||

{kind=link}