 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Volume 57, Number 12, December 2003, pp. 527-534 Allergen specific immunotherapy in nasobronchial allergy S V Joshi, D M Tripathi,* H L Dhar** MSc, Sr. Technical Officer; *PhD, Hon. Allergologist; **BSc, MBBS, PhD, DHA, FCAI, FICG; Medical Research Centre, Bombay Hospital Trust, Mumbai - 400020, India. Accepted 21-12-2003 Code Number: ms03043 ABSTRACT
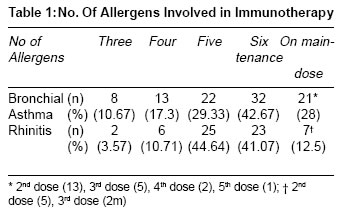
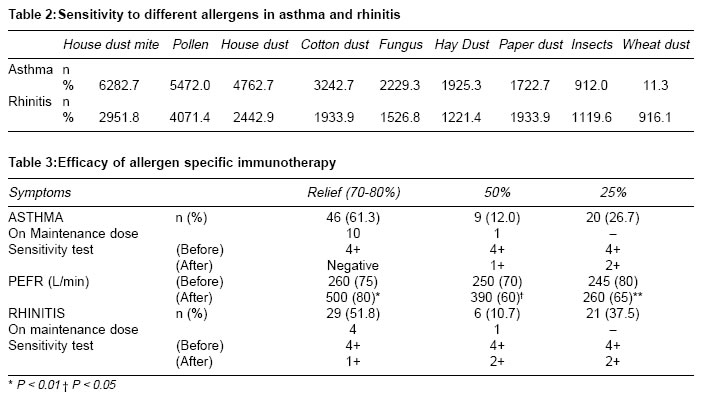
Background: More than one antigen have been used for immunotherapy of allergic disorders. So far less than five antigens have been employed with variable results. AIM: To evaluate effect of multiple antigens up to six in the immunotherapy of nasobronchial allergy. INTRODUCTION Specific immunotherapy (SIT) is one of the treatment modalities available to medical profession for allergic disorders. Immunotherapy which is also known as hyposensitization or desensitization was developed long before immune mechanism involving IgE antibodies was defined. It was introduced by Noon in 19111 by inoculating pollen extracts in cases of hay fever. Literature reveals that different methods have been applied from time to time viz. inhalation method2,3 in asthma sensitive to house dust mite (D pt) and Rinkle method in pollen hay fever.4 Later Ohman and Bousquet et al5,6 used the allergen immuno-therapy in asthma and allergic diseases. In India, an array of workers7-11 reported hyposensitization in respiratory allergy and asthma. New understanding of classical allergic diseases such as rhinitis and asthma has underlined their multiple pathogenesis and wide clinical spectrum.12 The treatment of allergic diseases involves reducing severity of symptoms by immunomodulating the disease process itself.13-15 The purpose of this study, was to have detailed information about the efficacy of allergen specific immunotherapy with mixture of antigens in naso-bronchial allergies. MATERIAL AND METHODS Five hundred cases of various allergic diseases viz. urticaria, rhinitis and asthma referred to the Department of Allergy, Bombay Hospital were screened. Patients have been selected on the basis of following criteria: clinical history, symptoms present for at least 3 years; age of the subject between 10 to 50 years and positive skin prick test. Criteria for immuno-modulation for asthma: documented IgE mediated asthma, failures in allergen avoidance and moderate to severe clinical manifestations. Based on these criteria, allergen specific immunotherapy was initiated in 200 perennial allergic subjects. All the 131 cases (56 rhinitis; 75 asthma) included in this study had given consent. Raised total IgE was found in all the subjects. Allergen source: Dusts were collected from patient's surroundings and were subjected to microscopic examination for presence of mites. Mites were isolated from bed and floor dust and were cultured in laboratory using standardized procedures. Pollen raw material was collected from specific plants species. The polliniferous material was then processed to achieve a purity of 99%. After confirming the purity and identity the purified pollen raw material was defatted with petroleum ether (40-60degrees C) to remove fatty substances. The allergenic raw material was stored at - 20 degree C and was used for preparation of allergen extracts. Identified fungal strains were innoculated and cultured in the Lab. The sporulated mass was used for production of raw material used for preparation of allergen extracts. All the allergens used in this study are approved by Drug Control of India and FDA for skin prick testing and hyposensitization treatment. In order to confirm the allergic manifestations, specific IgE for all the allergens was estimated by in vivo method (modified prick test) using allergens prevalent in the atmosphere consisting of dusts, house dust mites, pollens, insects, fungi and food. Allergen specific IgE is a better predictor of clinical allergy than total IgE levels or blood eosinophil counts. For assessing allergen specific IgE prick test is preferred method in comparison with various in vitro tests viz. RAST and QUIDEL. Prick test shows an 85% agreement with the above two methods.16 All the allergens were standardized and biological activity was determined in relation to histamine equivalent prick test in all individuals. This data was compared with allergen extracts routinely used for immunothrerapy. Allergen extracts were prepared in Cocas solution and were standardized on the basis of protein nitrogen units. Glycerophenol was used as an adjuvant. These extracts were subjected to undue toxicity test and sterility test before use for immunotherapy. Allergen extracts were formulated for SIT as per the prescription and specification on the basis of positive skin test results. Allergen extracts for SIT were grouped as either 1) Dusts and mite or 2) Pollen and fungi. For formulation of immunotherapy treatment extracts, endpoint titration method was used to determine a starting dose. In this method, allergens were diluted in serial dilution and each concentration was injected into the skin of the patient to find out allergen reactivity. The dilution which did not show any reaction was considered as starting/safe dose. These formulations were supplied by M/s Creative Diagnostic and Medicare Pvt. Ltd. in concentration of 1:25000, 1:2500, 1: 250 and 1: 50 w/v as per procedure of Allergo-Pharma, West Germany.17 Immunotherapy extracts were administered at different intervals as per recommended guideline provided by the company.6 Allergy shots were administered in incremental doses starting from lowermost concentration (1:25000) increasing at the interval of biweekly, weekly and fortnightly. Initial therapy was given for a period of 6-8 months until top tolerable dose was achieved. The maintenance therapy was initiated depending on the top tolerable dose. Duration of maintenance dose was one year and allergen shots were administered twice a month . In our study, all the patients received immunotherapy for three to six allergens. None was on single allergen therapy. The concentration of dust mite extract employed for immunotherapy was in the concentration of 0.2% w/v (1000 PNU) for Derp1 and 1500 PNU for Derf1. Allergens which are used for initial immunotherapy, the same were used for maintenance dosage without changing percentage composition (3-6 allergens). On completion of initial therapy, maintenance dose (two to four weeks interval) was advised to their family physicians and to every patient for maintaining the record of attack of asthma/rhinitis, severity of the symptoms and symptomatic treatment. These patients were advised to report back after completion of each vial for follow up. Baseline sensitivity test, peak expiratory flow rate along with symptoms were recorded. These parameters were noted after the treatment to substantiate the efficacy of immunotherapy. RESULTS Study group comprised of 75 asthmatics and 56 cases of rhinitis. In both the groups, number of allergens and mixture for immunotherapy formulation involved ranged from three to six (Table 1). Patients having rhinitis (44.64%) were found to be strongly positive for five different allergens (multiple allergens) compared to asthmatics (29.33%). Comparative figures for involvement of six different allergens were similar in asthma (42.67%) and rhinitis (41.07%). Among the patients who had positive history of asthma, sensitivity to house dust (62.7%) and house dust mite (HDM) (82.67%) were higher compared to house dust (42.86%) and HDM (51.78%) in rihinitis. However, sensitivity to pollen prevalent in the atmosphere of Mumbai18 was comparable in both the groups (72% and 71.43% respectively) (Table 2). One year follow up in cases of asthma showed that all of them completed the initial therapy . Out of the total (75), 13 were on second maintenance dose, 5 were receiving third dose and 2 with fourth dose and one patient having fifth dose. All rhinitis patients' (56), also completed the therapy. Of these, 5 were on second maintenance dose and two on third maintenance dose (Table 1). Significant symptomatic relief was observed in both the groups. The changes were assessed by way of skin sensitivity test, symptom score and peak expiratory flow rates (PEFR) in asthmatics while in rhinitis all parameters showed significant changes except PEFR (Table 3). Symptomatic therapy was also instituted in 5 _ 10% cases. DISCUSSION Immuno-therapy is indicated in patients with rhinitis and asthma caused by house dust mite and pollen in whom allergen avoidance and medications fail to control the symptoms.19,20 Allergen immunotherapy offers long standing relief from allergic diseases unlike mainstay pharmacotherapy, which merely counters the effects of inflammatory mediators. Recent insight into factors polarizing Th responses towards Th1 or Th2 is providing important new directions for refinement of SIT21 Our results show that the patients receiving SIT had significant symptomatic improvement in nearly 70% of cases (adults and paediatric group). Reports from Western countries showed symptomatic relief between 20-70% in nasobronchial allergy22 and 80%23 as well as 92 %24 in asthma. Similar success rates varying between 80% to 90% have also been reported by others in asthma25 and rhinitis.26 One report from India showed: overall seventy five percent improvement:66% in seasonal, 62% in irregular and 48% in perennial asthma.9 Tiwari7 in his study (10 to 40 year age group) also showed similar results (75%), however, respective percentages for seasonal, irregular and perennial asthma was low (55.5%, 44%, 40% respectively). In our series, therapy was planned on the basis of skin sensitivity using modified prick test which is very sensitive and specific16 and end point titration was attained using standardized allergens unlike previous studies from India7,9 employing intra-dermal tests. Intradermal tests even with proper negative and positive controls show a considerable number of false positive reactions and difficulty in interpretation.26 WHO committee on allergen skin testing does not approve intradermal testing as a routine procedure except in special cases.6 It has been stated that results of hyposensitization varies from place to place and good results depend on immunological state of the patient, degree of exposure to offending allergen and proper interpretation of skin test and methods used.27 Aqueous preparations of some allergens including Dermatophagoides pteronyssinus standerdized against WHO standard are extremely potent but severe local reactions have been reported28 However, with our purified and standardized aqueous extracts, no such reactions were observed. It was found that amongst multiple antigens employed for SIT, sensitivity to HDM (82.7%) was higher compared to HD (62.7%) &pollen (72.0%) in asthmatics. Telang et al11 reported positive intradermal tests for dust (54.7%), pollen (14.1%) and none for HDM. Such studies using multiple antigens have not been reported earlier except one study with less than 5 antigens.10 Other studies7,9 did not mention particular local allergens in rhinitis and asthma who received hyposensitization. Gaur & Gupta10 observed more than 50% response in 46.8% cases receiving immunotherapy with mixture of less than five antigens in one year. Our results show that 5-6 antigens (Table 1) were used in 72 % asthma cases and 85% in rhinitis during similar period. However, improvement (70-80%) was higher in asthma compared to rhinitis (51.8%) irrespective of number of allergens involved. Thus, multiple (mixture) allergen immunotherapy may be equally efficacious as monoallergen immunotherapy. Specific allergen immunotherapy was reported to be safe by Norman29 and subsequently used by others6,30 although different types of immunotherapy were recommended in allergic asthma viz. inhalation of allergen2,3 inoculation of allergen-antibody complexes.31 Immunotherapy was used in nasobronchial allergy7,32 as well as in pollinosis9,21,33 for chronic asthma. Lately Patterson30 used it in respiratory allergic diseases and Telang11 employed it in bronchial asthma. We observed that patients sensitive to HD and HDM showed significant improvement: 61.3% asthmatic patients experienced 70-80% symptomatic relief, 12% had 50% relief while 26.7% reported 25% relief. In subjects with rhinitis comparative figures were 51.8% (70-80% relief), 10.7% (50% relief) and 37.5% (25% relief) respectively. Efficacy of the allergen immunotherapy was also evidenced by the decline in allergen specific IgE antibodies by way of decreased skin test reactivity, reduced PEFR and reduction in medication. Immunotherapy has been reported to be beneficial with subjective clinical effect mainly in allergic rhinitis.27 In our study, patients with both asthma as well as rhinitis responded well to SIT. High efficacy in our study, might be attributed to uninterrupted therapy and use of standardized allergen extracts as reported by Johnstone34 in a study of pollinosis and pollen asthma. It is possible that continuation of therapy beyond 2-3 years might be more effective. Mital et al in a study comprising of 76 patients35 reported that 70% subjects with perennial asthma showed significant symptomatic relief with continuous treatment of SIT for 6 months. Complete to slight relief of symptoms was observed in 86.84% while 13.16% had no relief. In the present study, a mixture of five allergen extracts were used for immunotherapy in rhinitis (44.64%) and another six allergens for same condition (41.07%) for one year. In asthma figures were 29.33% and 42.67% respectively. The results were encouraging in both the groups. Earlier study carried out by Shivpuri36 showed positive results of hyposensitization with only mite allergen using intradermal test and with 0.01 ml of 1:2000 and prick test with 1:80 concentration. It has been observed that the degree of improvement increases with the period of regular immunotherapy. The efficacy of immunotherapy in our nasobronchial cases with multiple sensitivities has been shown to be beneficial though it has been reported that such patients (sensitive to pollen, dust mite, animal dander & mould) have more severe or more complex disease and do less well on allergen immunotherapy.37 We also observed significant improvement in PEFR, however, no such improvement was recorded in a study carried out at Trivandrum,37 difference could be due to different method employed. This study shows that SIT employing multiple allergens is as effective as monoallergen immunotherapy in bronchial asthma as well as in rhinitis in terms of reduced need of pharmaco-therapy. Since it is the first time up to six allergens have been used, precausions have been taken to assess the side effects as well as therapeutic benefits employing modified prick test, PEFR as well as clinical assessment based on set criteria viz. frequency of symptoms and drug requirement. These patients were followed up at frequent intervals. We intend to continue the immunization up to a period of three years for all subjects and look for prolonged period of remission. Attempts are being made to improve our understanding in the mechanism of action. REFERENCES 1. Noon L. Prophylactic inoculation against hay fever. Lancet 1911;1:1572-3. 2. Melillo G. Local immunotherapy by inhalation in allergic asthma. Respiration.1984;46:109-14. 3. Tari MG, Monti G. Immunotherapy by inhalation of allergen in powder in house dust allergic asthma. Berlin: XIV EAACI; 1989. 4. Van Metre TE Jr, Adkinson JF Jr, Amodio FJ, et al. A comparative study of effectiveness of the Rinkle method and the current standard method of immunotherapy for ragweed pollen hay fever. J Allergy Clin Immunol 1980;66:500-13. 5. Ohman JL. Allergen immunotherapy in asthma. Evidence of efficacy. J Allergy Clin Immunol 1989:84:133-43. 6. Busquet J, Lockey R, Mailing HJ and WHO panel members. Allergen immunotherapy: The therapeutic vaccine for allergic diseases. A WHO position paper. J Allergy Clin Immunol 1998;1024:558-61. 7. Tiwari UC. Results of hyposensitization in 100 cases of nasobronchial allergy due to local allergens. Asp Allergy & App Immunol Ed Mallick BB 1978;11:217-23. 8. Gupta KD, Kasliwal RM. The investigations, their techniques and methods of hyposensitization in respiratory allergy. Ind J Chest Dis 1960;2:90-4. 9. Dharam Prakash, Shivpuri DN. Results of desensitization in chronic asthma against local allergens. Asp of Allergy & App Immunol 1968;1:106-10. 10. Gaur SN, Gupta S. Clinical response of immunotherapy in case of nasobronchial allergy. Ind J of All & Appl Immunol 1996;10:65-8. 11. Telang JV, Mahashur AA, Shah SP, Kamat SR. Experience with intradermal antigenic tests and immunotherapy in bronchial asthma. JAPI J Assoc Physicians India 1986;34:189-90. 12. Hugh H, Windom & Alkis Togias. Rhinitis and asthma - manifestations of one disease. ACI international 2001;13:154-61. 13. Fahy JV, Fleming HE, Wong HH, et al. The effect of anti IgE monoclonal antibody on early and late phase responses to allergen inhalation in asthmatic subjects. Am J Resp Crit Care Med 1997;155:1828-34. 14. Boulet LP, Chapman KR, Cote J. et al Inhibitory effects of an anti IgE antibody E25 on an allergen induced early asthmatic response. Am J Resp Crit Care Med 1997;155:1835-40. 15. Casale TB, Bernstein L, Busse WW, et al. Use of anti IgE humanized monoclonal antibody in ragweed induced allergic rhinitis. J Allergy Clin Immunol 1997;100:110-21. 16. Ten RM, Klen JS, Frigas E. Allergy skin testing. Mayo Clinic Proc 1995;70:785-6. 17. Ganzer KG, Hamburg RK. Diagnostik and therapie allergischer - Krankheiten. Allergopharma Joachim. Posttach 1109:1-51. 18. Tripathi DM, Gupte SM, Vaz CJ. Aerobiological survey of Bombay Part II. Pollen and spore callender. J Ind All & Appl Immunol 1982;15: 43-8. 19. Abrahamson MJ, Puy RM, Weiner JM. Is allergen immunotherapy effective in asthma? A meta analysis of randomised controlled trials. Am J Respir Crit Care Med 1995;151:969-74. 20. Bousquet J, Hejjaoui A, Soussana M, Michel FB. Double blind, placebo controlled immunotherapy with mixed grass pollen allergoids. IV. Comparison of safety and efficacy of two dosages of a high molecular weight allergoid. J Allergy Clin Immunol 1990;85:490-7. 21. Rolland J, O'hehie RE. Targeting the allergen specific CD4+ T cell - strategies for improved allergen immunotherapy. ACI International 2001;13:170-7. 22. Tuft 1962. Clinical allergy. Lea & Febiger Philadelphia. Cited by Tiwari 1978 - Ref No.7). 23. Tuchinda M, Chai H. Effect of Immunotherapy in chronic asthmatic children. J All Clin Imm 1973;51:131. 24. Citren KM, Franklan AW, Sinclair JD. Quoted by Hobert LP, George WWJr. The role of injection therapy in allergic asthma. Postgraduate Med 1975;75:137-41. 25. Berstein L. Preventive therapy in the USA. In: Preventive therapy in asthma. Marley J, editor. Academic press; London: 1991. pp. 219-30. 26. Badhwar AK, Druce MM. Allergic rhinitis. In: Bush RK, editor. Clinical allergy. Med Clin North Am 1992;789-803. 27. Shivpuri DN, Agarwal MK. Studies on the allergenic fungal spores in Delhi, India Metropolitan area. J Allergy 1969;44:204-13. 28. Sheldon JM, Lovell RG, Mathews KP. A (1967) manual of Clinical Allergy. Pub W.B. Saunders Co. Phil, London. Cited by Shivpuri CR, Shivpuri DN: Re-evaluation of intradermal tests. Asp of All & Appl Immunol 1976;9:205-14. 29. Specific allergen immunotherapy for asthma. A position paper of the thoracic society of Australia & New Zealand and the Australian society of clinical immunology & allergy. MJA 1997;167:540-4. 30. Norman PS. Safety of allergen immunology. J Allergy Clin Immunol 1989;84:438. 31. Patterson R. The role of immunotherapy in respiratory allergic diseases. J Allergy Clin Immunol 1998;101:403-4. 32. Machiels JJ, Sommerville MA, Lebrun PM. Allergic bronchial asthma due to D pt. Hypersensitivity can be effectively treated by inoculation of allergen-antibody complexes. J Clin Invest 1990;85:1024. 33. Mital OP, Katiyar SK, Gupta MC, Singhal SK. Results of specific hyposensitization in cases of nasobronchial allergy. A subjective study. Asp of Allergy & AppI Immunol 1979;12:135-41. 34. Agnihotri MS, Singh AB. Observations in pollinosis in Lucknow with special reference to offending factors. Asp of Allergy & AppI Immunol 1971;5:135-40. 35. Johnstone DE. Study of role of antigen doses in treatment of pollinosis and pollen asthma. AMA J Dis Child 1957;94:1. 36. Shivpuri DN. House dust mite allergen in India. Asp of Allergy & Appl Immunol 1981;14:19-35. 37. Joshi M. Allergy, asthma & immunotherapy - An Indian perspective. Ind J All & AppI Immunol 2000;14:89-91. Copyright 2003 - Indian Journal of Medical Sciences. The following images related to this document are available:Photo images[ms03043t1.jpg] [ms03043t2.jpg] |
| |||||||||

{kind=link}
{kind=link}