 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Volume 57, Number 12, December 2003, pp. 535-542 Absence of Factor V Leiden (G1691A) mutation, FII G20210A allele in coronary artery disease in North India N Gupta, F Khan, M Tripathi, V P Singh, S Tewari,* V Ramesh,** N Sinha,* S Agrawal Department of Medical Genetics; *Department of Cardiology; **Department of Pathology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Rai Bareilly Road, Lucknow - 226014, India. Accepted 19-12-2003 Code Number: ms03044 ABSTRACT
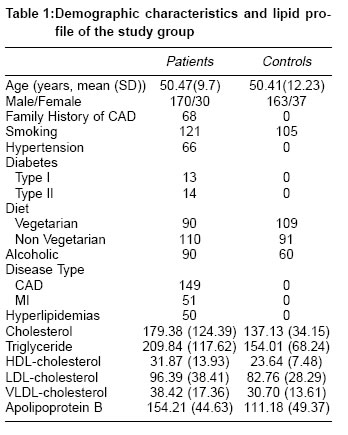
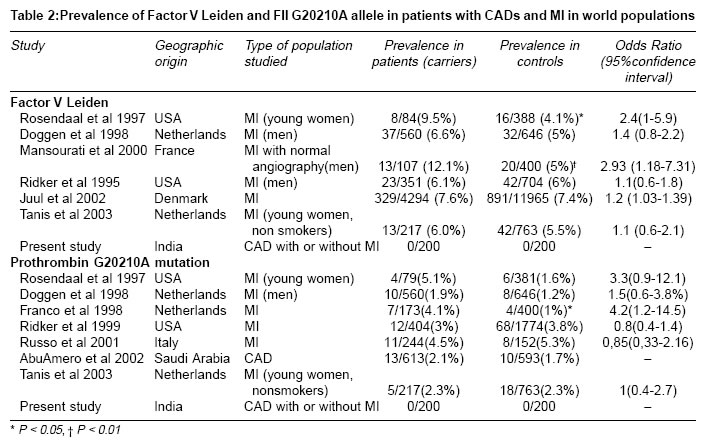
Background: Interaction between various genetic and environmental factors is associated with coronary artery diseases (CADs). Factor V Leiden mutation (FVL) and FII G20210A polymorphism are two recently described genetic factors with a propensity towards venous thrombosis, however, with a doubtful role in coronary artery disease and myocardial infarction. KEY WORDS: Coronary artery disease, Factor V Leiden (G1691A) mutation, Prothrombin gene (F IIG20210A) polymorphism. INTRODUCTION Coronary artery disease (CADs) is a complex multifactorial disorder exhibiting interaction between environmental and multiple genetic factors. The association between CADs and environmental factors has been thoroughly investigated but the role of genetic influences is still poorly understood. Various prothrombotic genetic markers that have been implicated in CADs are, -675 4G/5G polymorphism of the PAI-1 gene promoter, Pro33Leu polymorphism of the platelet glycoprotein IIIa gene, the C3550T polymorphism of the platelet glycoprotein Ib gene, the C677T polymorphism of methylene tetra hydro folate reductase (MTHFR) gene ,and the G10976A polymorphism of the factor VII gene, all showing inconsistent results.1Recently, two other polymorphisms, the G1691A mutation in the factor V gene (FVL) and the G20210 A mutation in the prothrombin gene have been found to be definitely associated with increased risk of venous thrombosis. However, the association of these two polymorphisms with arterial thrombosis is still controversial.1-3 Point mutation in factor V at 1691 position causes replacement of arginine by glutamine rendering FVa resistant to inactivation by activated protein C. Once the mutation occurs in factor V it leads to increased thrombin production hence raises the risk for venous thrombosis.G®A substitution at position 20210A in the 3'untranslated region in prothrombin gene is associated with raised plasma prothrombin. Mechanism of increased thrombosis is still not clear.2 Although these two polymorphisms have been reported in few cases of arterial thrombosis from different populations suggesting that the FVL mutation and G20210A polymorphism could be one of the risk factor for CADs and myocardial infarction (MI) however, results are still controversial.4-20 Only few studies are available on the prevalence of these two polymorphisms in Asians and their contribution to CADs. A recent study conducted on voluntary blood donors from India (Punjab) and, Indian tribes (Chorotegas, Bribri) have shown that the prevalence of heterozygote FVL is 1.3% in the population from Punjab while it is absent in Indian tribes, whereas prothrombin polymorphism was not seen at all.21 A recent study from Maharashtra describes FVL to be as prevalent as 10% especially in Vatalia Prajapati and Parsi normal population where as in MI the carrier frequency is as high as 4%.22 Garewal et al has shown the allele frequency in north Indian population for FVL is 1.9% where as prothrombin mutation is found to be not at all prevalent.23,24 In present study, the prevalence of these markers and their association with CADs is evaluated in North Indians from UP. MATERIAL AND METHODS Selection of cases and controls Sample collection Factor V Leiden mutation (FVL) detection PCR mixture consisted of 500 ng DNA, 25 pM/sample forward and reverse primers each, dNTP 300uM / sample, 1.5 units Taq polymerase (Banglore Genie) and 1 X PCR Buffer (20mM tris HCl, pH 8.4, 1.5mM MgCl2 &50 mM KCl) in final reaction volume of 30 ul. Reactions were carried out in DNA thermal cycler (MJ Research). Thermal profile consisted of 5 minutes denaturation at 940C followed by 30 cycles consisting of 1-minute denaturation at 940C, 30 seconds annealing at 610C and 30 seconds extension at 720C.Samples were then maintained at 720C for 10 minutes. 10 ul of 241 bp amplification products were then subjected to Hind III digestion with 1U/sample (GIBCO BRL) for 18 hours at 370C. Undigested and digested DNA products were size fractionated on 6.5% PAGE and visualized by ethidium bromide staining. Band sizes were analyzed for both digested and undigested DNA fragment by comparing them with 25 bp ladder (Amersham pharma). When subjects were homozygous for normal codon 506 corresponding to amino acid arginine (Arg / Arg), there was no restriction site for Hind III and fragment (241 bp) remained undigested. However, when subjects were homozygous for codon corresponding to glutamine at position 506 (Gln/Gln; Factor V Leiden mutation) a restriction site for Hind III was created on both the chromosomes that allowed the fragment to be completely digested into two fragments of 209 bp and 32 bp (latter was not visible on gel). When the subjects were heterozygous both patterns were visible, corresponding to undigested (241 bp) and digested (209 bp) amplified fragment as shown in Figure 1. Prothrombin Gene mutation (FII G20210A) detection RESULTS Two hundred patients with angiographically proven coronary artery disease (170 males, 30 females) and 200 normal controls (163 males, 37 females) were evaluated. The mean age of the patients was 50.47±9.7 while that of controls was 50.41±12.23. (Table 1) Lipids levels Factor V Leiden mutation FII G20210A mutation In both controls and CAD patients, we have not detected any mutation at factor V and prothrombin gene; hence no correlation against the risk factors (hyperlipidemias, smokers, diabetics) was possible. DISCUSSION Our results indicate that FVL and FII G20210A mutation were totally absent in the study population, therefore, no association of these factors with CAD in the subjects irrespective of age and in the subjects with or without the presence of major cardiovascular risk factors (obesity, diabetes, hypertension, and hypercholesterolemia) could be established among cases and controls from north India (UP). The FVL mutation is found in at least 90% of individuals with activated protein C resistance and is the commonest cause of venous thrombosis. Factor V Leiden mutation is inherited in an autosomal dominant manner and shows significant heterogeneity in the prevalence of FVL mutation amongst the ethnic groups, being common among Europeans and rare among Asians and Africans.28 The overall prevalence of FVL mutation is 3-7% in white women. It shows variable penetrance in the European population, ranging from a carrier rate of 0% in Italians to 14% in Greeks. The remarkably high prevalence of FVL in European population and its origin from a single founder mutation argues strongly against a significantly adverse effect on life expectancy.29 However, a very low prevalence was found in few Asian population viz. Tharu (1/230), Thailand (1/500). The prevalence among Indians from Maharashtra has been found to be 2.4%-10.5%.22 Homozygosity for FVL confers increased risk for venous thromboembolism at a younger age. Factor V heterozygotes have seven times higher risk of thrombosis than in general population. Heterozygosity for FVL is present in 20%-40% of western population with thromboembolic disease. The association between factor V Leiden and CADs remains controversial with some of the studies showing increased risk of CAD in carriers of FVL, in combination with other major cardiovascular risk factors4,5,11 while others failed to show any such association.6-8,12 (Table 2) FII G20210A allele is common among healthy whites and is rare in Asians and Africans. It has an allele frequency of around 1.2% in European population. Like factor V, same founder effect has been demonstrated for this mutation also, suggesting that these mutations occurred after the separation of non-Africans from Africans and after the divergence of whites and Asians.30 It seems biologically possible that the higher prothrombin levels may confer an increased risk of arterial disease. However, studies that attempt to establish the relation between the presence of 20210A prothrombin allele and CAD have yielded conflicting results, some show positive association especially in the presence of major cardiovascular risk factors9-12 while others studies from different population have failed to establish such link.13-20,31 (Table 2) Conflicting studies on the contribution of the coagulation defect seems to depend on the type of the population studied, with positive association in specific subgroups of young women, smokers and patients with metabolic risk factors or patients with normal coronary angiographies. Our results show that these two polymorphisms are not at all present in our population and, do not have any effect over CADs even in the presence of risk factors suggesting that these genetic variations could not be considered a major risk factor for either CADs or MI. The reasons for these results could be that the studies showing the positive associations have mainly been conducted in Caucasians who already manifest these genetic factors at a higher frequency in the general population. Hence the positive association may be because of the presence of major cardiovascular risk factors, suggesting that the interaction of these factors with common environmental factors like dietary habits, oral contraceptives, hypertension, smoking, diabetes, obesity is the precondition of the role of such factors in a given population. We propose that in complex, polygenic, multifactorial disorder like MI, the role of inherited predisposition to thrombosis due to factor V mutation and prothrombin gene mutation is relatively weak in itself and more so ever weaker than the traditional risk factors. Hence, laboratory screening for the above conditions in patients who present with arterial thrombosis should be considered of little value. In contrast, these patient might be investigated to detect antiphospholipid antibodies, hyperhomocystinemia, and dysfibrinogenemia, which are frequently associated with arterial thrombosis. In conclusion, our findings in this case control study reveals no association of FVL mutation and prothrombin gene mutation in genetic predisposition to CADs and MI in north Indian population. The discrepancies in studies relating to FVL mutation and FII G20210A allele to CADs may be due to difficulties in estimating low allelic frequency in general population. However, patients and normal individuals from other parts of the country need to be studied before evaluating the exact role of these mutations in CAD patients from India. REFERENCES 1. Lane AD, Grant PJ. Role of hemostatic gene polymorphisms in venous and arterial thrombotic disease. Blood 2000;95:1517-32 2. Poort SR, Rosendaal FR, Reitsma PH, Bertina RM. A common genetic variation in the 3'-untranslated region of the prothrombin gene is associated with elevated plasma prothrombin levels and an increase in venous thrombosis. Blood 1996;88:3698-703. 3. De Stefano V, Martinelli I, Mannucci PM, Paciaroni K, Chiusolo P, Casorelli I et al. The risk of recurrent deep venous thrombosis among heterozygous carriers of both factor V Leiden and the G20210A prothrombin mutation. N Engl J Med 1999;341:801-6. 4. Rosendaal FR, Siscovick DS, Schwartz SM, Beverly RK, Psaty BM, Longstreth WT, et al. Factor V Leiden (resistance to activated protein C) increases the risk of myocardial infarction in young women. Blood 1997;89:2817-21. 5. Mansourati J, Da Costa A, Munier S, Mercier B, Tardy B, Ferec C, et al. Prevalence of factor V Leiden in patients with myocardial infarction and normal coronary angiography. Thromb Haemost 2000;83:822-5. 6. Ridker PM, Hennekens CH, Lindpaintner K, Stampfer MJ, Eisenberg PR, Miletich JP. Mutation in the gene coding for coagulation factor V and the risk of myocardial infarction, stroke, and venous thrombosis in apparently healthy men. N Engl J Med 1995;332:912-7. 7. Cushman M, Rosendaal FR, Psaty BM, Cook EF, Valliere J, Kuller LH, et al. Factor V Leiden is not a risk factor for arterial vascular disease in the elderly: results from the Cardiovascular Health Study. Thromb Haemost 1998;79:912-5. 8. Juul K, Tybjaerg-Hansen A, Steffensen R, Kofoed S, Jensen G, Nordestgaard BG. Factor V Leiden: The Copenhagen City Heart Study and 2 meta-analyses. Blood 2002;100:3-10. 9. Rosendaal FR, Siscovick DS, Schwartz SM, Psaty BM, Raghunathan TE, Vos HL. A common prothrombin variant (20210 G to A) increases the risk of myocardial infarction in young women. Blood 1997;90:1747-50. 10. Franco RF, Trip MD, Ten H, van den Ende A, Prins MH, Kastelein JJ, et al. The 20210 G—>A mutation in the 3'-untranslated region of the prothrombin gene and the risk for arterial thrombotic disease. Br J Haematol 1999;104:50-4. 11. Doggen CJ, Cats VM, Bertina RM, Rosendaal FR. Interaction of coagulation defects and cardiovascular risk factors: increased risk of myocardial infarction associated with factor V Leiden or prothrombin 20210A. Circulation 1998;97:1037-41. 12. Gardemann A, Arsic T, Katz N, Tillmanns H, Hehrlein FW, Haberbosch W. The factor II G20210A and factor V G1691A gene transitions and coronary heart disease. Thromb Haemost 1999;81:208-13. 13. Corral J, Gonzalez-Conejero R, Lozano ML, Rivera J, Heras I, Vicente V. The venous thrombosis risk factor 20210 A allele of the prothrombin gene is not a major risk factor for arterial thrombotic disease. Br J Haematol 1997;99:304-7. 14. Russo C, Girelli D, Olivieri O, Guarini P, Manzato F, Pizzolo F, et al.G20210A prothrombin gene polymorphism and prothrombin activity in subjects with or without angiographically documented coronary artery disease. Circulation 2001;103:2436-40. 15. Coulet F, Godard V, Verdy E, Soubrier F. Lack of association of the prothrombin gene variant G20210A with myocardial infarction in Caucasian males. Thromb Haemost 2000;83:796-7. 16. Croft SA, Daly ME, Steeds RP, Channer KS, Samani NJ, Hampton KK. The prothrombin 20210A allele and its association with myocardial infarction. Thromb Haemost 1999;81:861-4. 17. Tanis BC, Bloemenkamp DG, van den Bosch MA, Kemmeren JM, Algra A, van de Graaf Y, et al. Prothrombotic coagulation defects and cardiovascular risk factors in young women with acute myocardial infarction. Br J Haematol 2003;122:471-8. 18. Eikelboom JW, Baker RI, Parsons R, Taylor RR, van Bockxmeer FM. No association between the 20210G A prothrombin gene mutation and premature coronary artery disease. Thromb Haemost 1998;80:878-80. 19. Prohaska W, Schmidt M, Mannebach HM, Gleichmann U, Kleesiek K. The prevalence of the prothrombin 20210G—>A mutation is not increased in angiographically confirmed coronary artery diaease. Thromb Haemost 1999;81:161-2. 20. Ridker PM, Hennekens CH, Miletich JP. G20210A mutation in prothrombin gene and risk of myocardial infarction, stroke, and venous thrombosis in a large cohort of US men. Circulation 1999;99:999-1004. 21. Herrmann FH, Sanchez LS,Schroder W,Grimm R,Schuster G, Arce J, et al. Prevalence of molecular risk factor FV Leiden, FVHR2, FII20210G—>A and MTHFR 677C—>T in different populations and ethnic groups of Germany, Costarica, and India. Int J Hum Genet 1:33-9. 22. Pawar AR, Shetty S, Ghosh K, Mohanty D. How old is factor V Leiden mutation ? Thromb Hemost 2001;86:1591-2 23. Garewal G, Das R, Trehan U. Factor V Leiden: Prevalence in the indigenous population and cases of thrombosis in North India. Br J Haematol 1997;97:940. 24. Garewal G, Das R, Ahluwalia J, Mittal N, Varma S. Prothrombin G20210A is not prevalent in North India. J Thromb Haemost 2003;1:2253-4. 25. Olerup O, Zetterquist H. HLA-DR typing by PCR amplification with sequence-specific primers (PCR-SSP) in 2 hours: an alternative to serological DR typing in clinical practice including donor_recipient matching in cadaveric transplantation. Tissue Antigens 1992;39:225-35 26. Gandrille S, Alhenc-Gelas M, Aiach M. A rapid screening method for the Factor V Leiden Arg 506 Gln mutation. Blood Coagulation Fibrinolysis 1995;6:245-8. 27. Thakur S, Agarwal S, Khan F, Phadke SR, Pradhan M, Pandey M, et al. Factor V Leiden mutation (G1691A) in women with recurrent spontaneous abortions from North India. Obs Gynae today 2003 (in press). 28. Rees DC, Cox M, Clegg JB. World distribution of factor V Leiden. Lancet 1995;346:1133-4. 29. Zivelin A, Griffin JH, Xu X, Pabinger I, Samama M, Conard J, et al. A single genetic origin for a common Caucasian risk factor for venous thrombosis. Blood 1997;89:397-402. 30. Zivelin A, Rosenberg N, Faier S, Kornbrot N, Peretz H, Mannhalter C, et al. A single genetic origin for the common prothrombotic G20210A polymorphism in the prothrombin gene. Blood 1998;92:1119-24 31. Amero AKK, Wyngaard CA, Kambouris M, Dzimri N. Prevalence of the 20210G—>A prothrombin variant and its association with coronary artery diseasein a middle eastern Arab population. Arch Pathol Lab Med 2002;126:1087-90. Copyright 2003 - Indian Journal of Medical Sciences. The following images related to this document are available:Photo images[ms03044t1.jpg] [ms03044t2.jpg] |
| |||||||||

{kind=link}
{kind=link}