 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Science Vol. 58 No. 1, January 2004 , pp. 3-9 Evaluation of Serum Steroid Hormones in Schizophrenic Patients M Taherianfard , M Shariaty Ebne Sina Hospital and School of veterinary Medicine of Shiraz University
Accepted Date 25-01-04 Code Number: ms04001 ABSTRACT BACKGROUND: Recent studies have implicated the abnormalities in the g-aminobutyric acid (GABA) neurotransmmiter system in the pathophysiology of schizophrenia. There are also evidences indicating that steroids of central or peripheral origin may modulate GABAergic system through direct interaction with the GABAA receptor complex. These raise the possibility that alternations in serum steroid hormones may contribute to the pathophysiological process in the schizophrenia. AIMS: The purposes of this study were first, to determine whether alternations in steroid serum levels occur in schizophrenic patients, and secondly to determine whether such alternations normalize with clinical improvement. Methods and material: serum concentrations of testosterone (T), estradiol (E), progesterone (P) and cortisol (C) were determined in male schizophrenic patients (N=49) before treatment, during treatment and after recovery and in age-matched healthy male subjects (N=17). All steroid hormones were assayed by ELISA method. Statistical analysis used: Differences in steroids concentrations between groups were assayed by One-Way Analysis of Variance (ANOVA), followed by Tukey's post hoc test. The level of significance was considered at P<0.05. RESULTS AND CONCLUSION: the serum concentrations of E, P and C were significantly (P<0.05) lower in male schizophrenic patients in all three stages of the study, compared with healthy subjects. serum concentrations of T were significantly (P<0.05) lower in male schizophrenic patients before and during treatment, but not after recovery, compared with healthy subjects. These findings support the occurrence of abnormal steroid concentrations in schizophrenic patients and suggest that lower T level in this disorder is related to the illness and normalizes with remission, while trait-related factors may contribute to lower serum E and C levels in schizophrenia. KEY WORDS: Schizophrenia, GABAergic, Testosterone, Estradiol, Progesterone, Cortisol. Introduction Schizophrenia is a disabling brain disease of unknown etiology and pathogenesis.1 Recent biochemical studies have linked schizophrenia to alteration in g-aminobutyric acid (GABA) neurotransmission in the prefrontal cortex of schizophrenic brain.2-4 some investigators have suggested that reduced inhibitory GABAergic tone in the limbic cortical region may contribute to the schizophrenic symptoms.5 moreover, postmortem studies have indicated a widespread upregulation of GABAA receptor binding activity throughout most subregions of the hippocampal formation of and in layer II of the anterior cingulate cortex of schizophrenic brain.4,6 Furthermore, the action of benzodiazepines (BZ), widely used in psychotic patients, are mediated through binding to a specific binding sites in the brain which alter the responsiveness of the GABA.7 Taken together, the above findings implicate disturbed GABA neurotransmission occur in schizophrenia. There are also evidences that some steroid derivatives of progesterone (P), testosterone (T) and glucocorticoids can alter physiological responses to GABA, apparently through direct interaction with the GABA receptors.8-11 This together with the substantial evidence pointing to disturbances in GABA system in the pathophysiology of schizophrenia raise the possibility that abnormalities in steroid hormones may confer susceptibility to schizophrenia. Interestingly, recent studies have indicated a role for gonadal steroids as possible contributors to understanding the sex differences in the clinical features in schizophrenia.12 In this regard, estrogen may contribute to later onset and less severe course of illness in women.13 Furthermore, it has been suggested that gonadal hormone withdrawal in postmenopausal women may predispose to schizophrenia by reducing brain dopamine receptors and producing an imbalance of GABAA receptors in the output pathways of the striatum.14 Few studies have examined steroid hormones in male schizophrenics indicating lower serum T levels in male schizophrenic subjects.15 However, it is unknown whether such changes are due to long-term use of antipsychotics or the mental illness itself. On the other hand Brown et al. pointed out that schizophrenia in late adolescence and early adulthood was accompanied by hypothalamo-pitutary-gonadal (HPG) axis abnormalities.16 So the aim of present study was undertaken first, to determine whether HPG abnormalities in schizophrenic patients lead to alternation in serum steroids, and secondly to determine whether such alternations, if any, normalize with clinical improvement.
Material and Methods
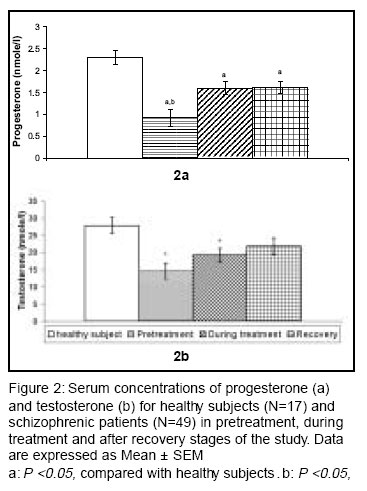
Subjects This study was carried out on 49 physically healthy male schizophrenic patients recruited through neurology unit of Ebne Sina Hospital of Shiraz and 17 healthy subjects who are similar in age and sex. Diagnosis of schizophrenia was based on clinical criteria including thought disorder, delusion, persecution, grandeur and hallucination which was confirmed by using the Structured Clinical Interview for DSM-IV Axis-I disorders-Patient Edition (SCID/IP),17 administered by a research psychiatrist or a trained clinical psychologist. They met the following inclusion/exclusion criteria: age between 17 to 30 years, Schizophrenia was the primary diagnosis in all patients (71% familiar and 29% non-familiar) more than 62% were graduated and about 82% of them were addicted to cigarette. Patients were excluded if they had a history of mental retardation. The male healthy subjects had no current, past or family history of psychiatric disorder. Patients were studied in three stages: 1- At first admission before treatment and drug free patients defined as "pretreatment", 2- Three week after beginning of treatment patients were considered as "during treatment" and Measurements of steroid concentrations After the subjects had fasted overnight, blood samples were collected at 8 a.m. from healthy subjects and the same schizophrenic patients at three stages: pretreatment, during treatment and after recovery. Patients were treated with flurozepam, triazolam or diazepam plus antipsychotic drugs. Serums were prepared from clotted blood and stored at -20°C until use. Serum concentrations of cortisol (C), estradiol (E), T and P were assayed in triplicate by ELISA using Medix biotechnology industrial kit, the accuracy of test was 0.01 nmole/ml. All experimental procedures were conducted according to the manufacturer's instruction. Statistical analysis Differences in steroids concentrations between groups were assayed by one-way analysis of variance (ANOVA), followed by Tukey's post hoc test. The level of significance was considered at P<0.05, degree of freedom 3 and confidence interval 95%. The statistical analyses were performed using the SPSS (version 10.0) statistical package. Results Subjects The mean ages of the subject groups studied were 24 ± 4.9 and 26 ± 4.6 for schizophrenic and healthy subjects, respectively. There were not statistically significant (P>0.05) differences in age between schizophrenic and healthy subjects. Serum Steroid levels The serum concentrations of E was significantly [F3=8.36, (P<0.001)] lower in schizophrenic patients in all 3 stages of disease compared with healthy subjects. In schizophrenic patients, no significant (P>0.05) differences were found between pretreatment, during treatment and recovery stages in the serum levels of E (Figure 1). The serum concentrations of C was significantly [F3=4.36, (P=0.0073)] lower in schizophrenic patients in all 3 stages of disease compared with healthy subjects. In schizophrenic patients, no significant (P>0.05) differences were found between pretreatment, during treatment and recovery stages in the serum levels of C (Figure 1). The serum concentrations of P were significantly [F3=12.1, (P<0.001)] lower in schizophrenic patients during the entire course of the study compared with healthy subjects (Figure 2a). In schizophrenic patients, serum P levels during treatment and recovery stages were significantly (P<0.05) higher compared with pretreatment stage. There were no significant (P>0.05) differences in P concentrations between during treatment and recovery stages (Figure 2a). The serum concentrations of T were significantly [F3=5.83, (P=0.0014)] lower in schizophrenic patients in pretreatment and during treatment stages, but not after recovery, compared with healthy subjects (Figure 2b). In schizophrenic patients, serum T concentrations were significantly (P<0.05) higher after recovery compared with pretreatment stage, but not in comparison to during treatment. No significant differences were found between the pretreatment and during treatment stages in serum T concentrations (Figure 2b). Discussion The principal finding of this study is the evidence of reduced C, E, P, and T concentrations in serum of male schizophrenic patients compared with healthy subjects. The lower steroid serum levels in schizophrenic patients could not be accounted for by age or medication intake. Thus, the current findings provide a strong support for the idea that abnormal steroid serum levels occur in schizophrenia and may be involved in the pathophysiological process of schizophrenia, at least in male schizophrenics. This is consistent with the report of Boss et al suggesting that gonadal hormone withdrawal by reducing brain dopamine receptors and imbalance of GABAA receptors in the out put pathways of the striatum may predispose the subjects to schizophrenia and dyskinesia.14,18 To our knowledge, this is the first longitudinal study to evaluate both gonadal and adrenal steroids in the same schizophrenic patients before treatment, during treatment and after recovery. This provides a strategy to assess the extent to which the episode of the illness, medication and/or trait-related phenomena contributes to alterations in steroid serum levels in schizophrenia, if any. Our findings of lower T concentrations in male schizophrenic patients are in agreement with previous findings reported by Rasanen et al.15 Significantly lower serum T in male schizophrenic patients before treatment compared to healthy subjects and its increase to a level comparable to those in healthy subjects after remission suggests that lower T concentration in schizophrenics may be consequences of the illness and pscyhotic symptoms which normalized with clinical improvement. A possible effect of medication on T level can be ruled out by the finding of no significant differences in T before and during treatment in schizophrenic patients. In contrast, lower than normal C and E serum levels in schizophrenic patients before treatment persist after BZ treatment and after recovery. This suggests that abnormalities in these steroid levels in male schizophrenic patients may be trait-related. Serum P levels significantly increased in schizophrenic patients following BZ treatment, compared with before treatment. Serum from the same patients after recovery exhibited P levels similar to those during treatment, but significantly lower than healthy subjects. These findings implicate an effect of BZ administration on serum P levels. One possible mechanism by which BZ may affect P levels may be attributable to their action on peripheral-type benzodiazepine receptors (PBR). It has been previously shown that PBR are extremely abundant in steroidogenic cells.19,20 Furthermore, Papadopoulos et. al, have suggested that BZ via binding to PBR stimulate steroidogenesis.21-23 Therefore, increased P levels following BZ treatment in schizophrenic patients may be due to their action on PBR and promoting cholesterol transport to the inner membrane and in turn, its conversion to progesterone.
In conclusion: The current findings support the occurrence of abnormal steroid levels in schizophrenia and suggest a possible role for steroids in the psychopathology of schizophrenia. Stevens reported that onset of schizophrenia occurs during the reproductive period in more than 80% of those affected.24 The exact mechanism(s) by which the observed alterations in steroid levels occur in schizophrenia is unknown. These abnormalities may occur as a primary changes following deficient HPG function16 or secondary to other neuronal disturbances reported in schizophrenia. Clearly, further study is necessary to clarify the pathophysiological basis for the altered steroid levels in schizophrenia. Halbreich and Kahn were suggested that may be a key role for future applications of specific estrogens for improved treatment of schizophrenics. `Atypical' antipsychotics definitely improved the benefit/risk ratio of treatment of schizophrenic patients.25
Acknowledgements The authors would like to thank Drs. M. Emamghoreishi, B. Farashbandi, M. Sajadi, and A. Fakor for clinical diagnosis of patients during the course of study and Mr. Khatei for his assistance in blood collection from subjects entered in the study. References
Copyright by The Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04001f1.jpg] [ms04001f2.jpg] |
| |||||||||

{kind=link}
{kind=link}