 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
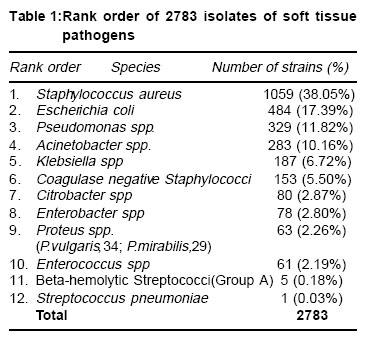
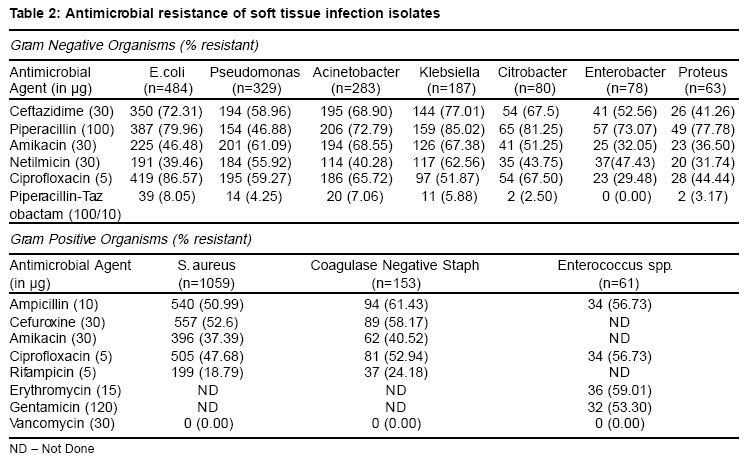
Indian Journal of Medical Science Vol. 58 No. 1, January 2004 , pp. 10-15 Bacteriological and Antimicrobial Susceptibility Profile of Soft Tissue Infections from Northern India S Mohanty, A Kapil,* B Dhawan, B K Das* MD; Senior Research Associate; Additional Professor; Associate Professor; Department of Microbiology, AIIMS, New Accepted Date 20-01-04 Code Number: ms04002 ABSTRACT BACKGROUND: Soft tissue infections require a judicious combination of antimicrobial therapy in addition to surgical debridement to limit tissue loss and preserve life. AIMS: To study the bacterial etiology of soft tissue infections and their antimicrobial susceptibility pattern. Settings and design: A single institutional retrospective study of one year duration from January to December 2002. MATERIALS AND METHODS: A total of 5039 consecutive pus samples received in the Bacteriology Laboratory was analyzed from the records. Results: There were a total of 2783 bacterial isolates comprising of 1504 gram negative bacilli and 1279 gram positive cocci. Staphylococcus aureus was the commonest isolate followed by Escherichia coli and Pseudomonas species. Methicillin resistance in S. aureus was found to be 38.56%, high level aminoglycoside resistance was observed in 53.3% enterococci and 66.75% of the gram negative bacilli were extended spectrum beta-lactamase producers. Rifampicin and vancomycin showed best activity for S. aureus; for gram-negative bacilli, piperacillin-tazobactam combination showed best activity. CONCLUSIONS: Continuous monitoring of antimicrobial susceptibility pattern in individual settings together with their judicious use is emphasized to minimize emergence of drug resistant bacteria. KEY WORDS: Soft tissue infection, Antibiogram, Beta lactams, Methicillin resistant Staphylococcus aureus, High level aminoglycoside resistance. Introduction Skin and soft tissue infections (SSTIs) are a common type of infection that may contribute to longer hospital stays, significantly increase the cost of medical care, and are likely to have an important role in the development of antimicrobial resistance.1,2 Most of these infections are superficial and readily treated with a regimen of local care and antibiotics. However, soft tissue infections involving deeper layers like fascia and muscle can rapidly progress to systemic sepsis and prove fatal.3 These are the type of infections that require a wise choice of antimicrobials in addition to aggressive surgical debridement to limit tissue loss and preserve life.1,3 Since initial antimicrobial therapy usually remains empiric, it is important to know, the prevailing susceptibility patterns of bacterial isolates at individual institutions by routine surveillance. With the recent emergence and spread of resistant Gram-positive cocci and Gram-negative bacilli including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin resistant enterococci (VRE) and extended spectrum beta-lactamase (ESBL) producing bacilli, SSTIs have posed a great challenge to primary care practitioners. This retrospective study was therefore carried out to investigate the agents responsible for soft tissue infections in a tertiary care hospital of India and study their antimicrobial susceptibility pattern to guide empirical therapy. Materials and Methods Specimens This retrospective analysis included 5039 consecutive pus samples obtained from patients admitted to various specialities of Antimicrobial susceptibility testing Antimicrobial sensitivity was performed on Mueller-Hinton agar (Hi-Media, India) by the standard disk diffusion method recommended by the National Committee for Clinical Laboratory Standards. (NCCLS).5 Standard strains Escherichia coli ATCC 25922, Staphylococcus aureus ATCC 25923 and Pseudomonas aeruginosa ATCC 27853 were used as controls. Organisms were tested for antibiotics based on their expected primary activity. The diameter of the zone of inhibition of growth was recorded and interpreted as susceptible or resistant by the criteria of NCCLS.5 Organisms with "intermediate" levels of resistance were included in the percentage of resistant organisms for final analysis. Detection of ESBL All gram- negative bacilli (GNB) were tested for ESBL production by a double disc diffusion method recommended by NCCLS.5 Klebsiella pneumoniae 700603 was used as a control. An enhanced zone of inhibition with a difference of ³5 mm around the ceftazidime-clavulanic acid disk as compared to the ceftazidime disk alone was interpreted as presence of ESBL. Detection of Methicillin resistance Staphylococcus spp. were tested for methicillin resistance by using 1µg oxacillin disk.5 The S. aureus strains ATCC 25923 and WHO-2 were used as negative and positive controls respectively. Agar plates were incubated at 350C and read at 48 hours of incubation. Organisms were deemed methicillin resistant when zone of inhibition was £10 mm and £17mm for S. aureus and coagulase negative Staphylococci respectively. Detection of VRE Enterococci were tested for vancomycin resistance by the vancomycin disk (30µg) and screen agar containing vancomycin 6µ/ml.5 A vancomycin screen agar (6µg/ml) was also put up to detect vancomycin intermediate isolates of Staphylococcus. Enterococcus species resistant to gentamicin (120µg) disk were termed high level aminoglycoside resistant (HLAR). Results Of the 5039 pus samples received for culture during the study period, 2437 (48.36%) were culture positive, while 1831 (36.33%) samples were culture negative. Diphtheroids, environmental bacillus species and > 3 agents (contaminants) were grown in 771 (15.30%) samples which were not processed further. Among the 2437 culture positive samples, the number of bacterial isolates obtained were 2783 (2091 had a single pathogen and 346 had 2 types of bacteria). Of the 2783 clinical isolates, there were 1504 (54.04%) gram negative bacilli and 1279 (45.96%) gram positive cocci (Table 1). The top six organisms accounted for nearly 90% of all pathogens. In the 346 samples where mixed infection was found, the combination of S. aureus and E.coli (57 samples) was commonest followed by S. aureus and Acinetobacter species (48 samples). Antimicrobial susceptibility a. Gram negative bacilli Resistance pattern of GNB to various antibiotics has been shown in Table 2. Of the 1504 isolates, only 218 (14.49%) were sensitive to all antibiotics. Extended spectrum beta-lactamase production was observed in 1004 (66.75%) isolates and ranged from 40.62% (lowest in Proteus species) to 76.34% (highest in Klebsiella species). For rest of the organisms, ESBL production was as follows : E. coli (72.31%), Acinetobacter spp (68.79%), Citrobacter spp (67.50%), Pseudomonas spp (58.79%) and Enterobacter spp, (51.28%). As regards piperacillin, best activity was detected for Pseudomonas species (resistance rate 46.88%) as compared to other gram negative bacteria (resistance rate 78.54%) demonstrating its better efficacy against Pseudomonas. Extended spectrum beta-lactamase producing bacilli were more resistant to other antibiotics compared to ESBl negative isolates (resistance rate 85.76% versus 23.43%). Overall, the gram negative bacilli showed good response to piperacillin-tazobactam. b. Gram positive organisms Resistance to methicillin was detected in 38.56% of S. aureus isolates and 31.16% of coagulase negative Staphylococci with cross-resistance to other beta-lactams i.e. ampicillin and cefuroxime (Table 2). Barring rifampicin, methicillin resistant S. aureus strains were significantly more resistant to other antibiotics compared to methicillin sensitive S. aureus strains (resistance rate 86.76% versus 26.56%). Discussion S. aureus, E. coli and Pseudomonas spp. are the top 3 pathogens in the present study similar to studies from India6 and outside2,7 where they frequently are amongst the top 5 pathogens isolated from skin and soft tissue infections in hospitalized patients. In the present study, prevalence of MRSA (38.56%) is higher than that reported from Nagpur (19.56%)8 and Vellore (24%)9 in India. However, it is comparable to that in United States and certain European countries10 where methicillin resistance was detected in 32.4% to 44.4% S. aureus isolates. Almost 87% of MRSA were resistant to other antibiotics like amikacin and ciprofloxacin which is a matter of great concern since options to treat these infections are drastically reduced. High resistance of MRSA to other antibiotics has been reported in previous studies also.8,9 Thus, at present vancomycin and rifampicin appear to be the drug of choice for treating MRSA infections. Alternate drugs like teicoplanin and quinupristine-dalfopristine have also shown promising results.2,7 As regards enterococci, more than half of the isolates (53.3%) were HLAR with the implication that the synergistic combination of beta-lactam plus aminoglycoside will not be active against them. Thus, the resistance pattern of enterococci needs to be monitored carefully. Gram negative bacilli demonstrated a high rate of ESBL expression (66.75%) which is comparable to that reported previously (68%) from India.11 Extended spectrum beta-lactamase positive isolates are frequently resistant to other antibiotics like quinolones and aminoglycosides11 which has been found in the present study also. Finding of more concern is the resistance of ESBL positive isolates to piperacillin-tazobactam (beta lactam-beta lactamase inhibitor) combination since the antibiotics of choice in the treatment of infection due to ESBL positive bacteria are limited to either these combinations or the carpapenems.12 The high rates of antibiotic resistance observed in the present study may be due to the fact that ours is a tertiary care hospital with widespread usage of broad spectrum antibiotics leading to selective survival advantage of pathogens. This is reinforced by the fact that in a previous study13 on nosocomial uropathogens done in our institute, a similar high rate of MRSA (23.8%), ESBL production (71.5%) and HLAR (70.17%) was reported. The susceptibility data collected in this study suggests that the most common organisms likely to be encountered in soft tissue infections are gram-positive cocci, notably S. aureus, many of them methicillin-resistant. Thus, any first line antibiotic treatment should be primarily directed against this pathogen. For coverage of gram negative bacteria, beta lactam-beta lactamase inhibitor combinations would be more useful. Use of mono drug therapy with cephalosporins, aminoglycosides and fluoroquinolones need to be guided by the sensitivity report. Lastly, continued monitoring of susceptibility pattern need to be carried out in individual settings so as to detect the true burden of antibiotic resistance in organisms and prevent their further emergence by judicious use of drugs. Reference
Copyright by The Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04002t2.jpg] [ms04002t1.jpg] |
| |||||||||

{kind=link}
{kind=link}