 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Science Vol. 58 No. 1, January 2004 , pp. 16-23 REDUCED MINIMUM INHIBITORY CONCENTRATION OF CHLORAMPHENICOL FOR SALMONELLA ENTERICA SEROVAR TYPHI S Mandal, M D Mandal, N K Pal Department of Bacteriology and Serology, Calcutta School of Tropical Medicine, C. R. Avenue, Kolkata - 700073, India.
Correspondence:
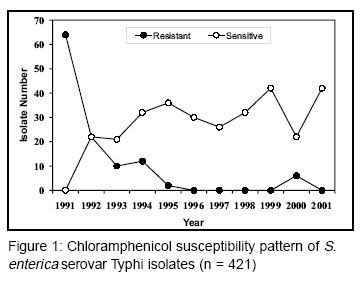
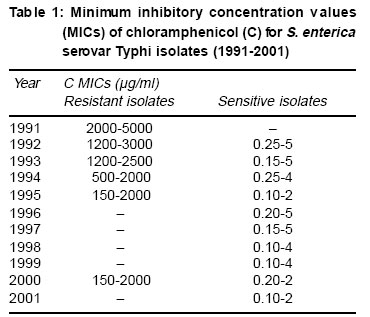
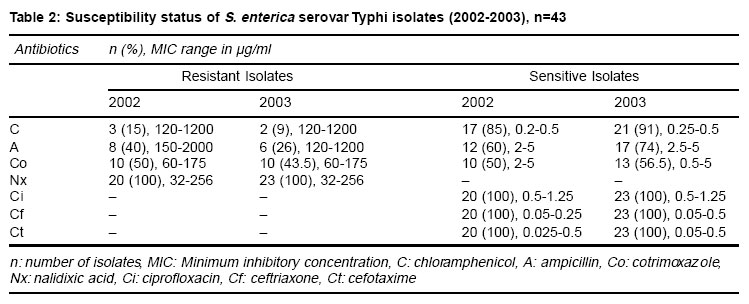
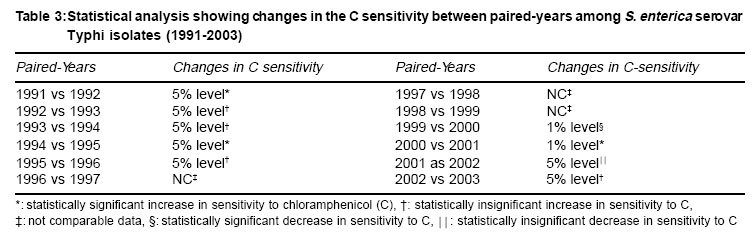
Nishith Kumar Pal, professor and Head, Department of Bacteriology and Serology, Calcutta School of Tropical Medicine, C. R. Avenue, Kolkata - 700073, India. Accepted Date 28-01-04 Code Number: ms04003 ABSTRACT BACKGROUND: Ciprofloxacin replaced chloramphenicol (C), the best choice of antibiotic in the treatment of enteric fever, when C-resistant enteric fever emerged and caused outbreaks in different parts of the world. C-sensitive S. enterica serovar Typhi emerged again due to withdrawal of the antibiotic pressure. AIMS: To assess the in vitro efficacy of C against Salmonella enterica serovar Typhi isolates (1991-2003). MATERIAL AND METHODS: A total of 464 blood culture isolates of S. enterica serovar Typhi were subjected to C susceptibility by disc diffusion and agar dilution methods using Mueller-Hinton agar. The antibiotic susceptibility of S. enterica serovar Typhi isolates obtained in the year 2002 and 2003 was determined using ampicillin, cotrimoxazole, ciprofloxacin, nalidixic acid, ceftriaxone and cefotaxime, in addition to C. Escherichia coli strain ATCC 25922 was used as the control. Changes in C sensitivity of the isolates were analyzed using c2 test with Yates correction. RESULTS AND CONCLUSIONS: All the isolates of 1991 were C-resistant with minimum inhibitory concentration values (MICs) of 2000-5000 mg/ml. In the following years decrease in frequency of C resistance was noticed: 1992 (50%), 1993 (32%), 1994 (27%) and 1995 (05%). The isolates of 1996-99 and 2001 were 100% C-sensitive. In 2000, sensitivity was also high (79%). The strains isolated in the year 2002 and 2003, showing reduced susceptibility of ciprofloxacin, were nalidixic acid resistant, but sensitive to the third-generation cephalosporins (ceftriaxone and cefotaxime). The MICs for C-sensitive isolates (1991-2003) ranged 0.1-5 mg/ml. Results suggest the necessity for re-evaluation of C therapy in typhoid fever. KEY WORDS: Chloramphenicol, Minimum inhibitory concentration, Salmonella enterica serovar typhi. INTRODUCTION Chloramphenicol (C) is usually bacteriostatic but may be bactericidal in high concentrations or against more susceptible microorganisms. It has a wide spectrum of activity against gram-positive and gram-negative bacteria. Antibiotic activity appears to result from inhibition of protein synthesis of bacterial cells. C binds to the 50S subunit of bacterial ribosomes, which inhibits peptide bond formation. The dosage of C in typhoid fever (TF) is 50 mg/kg/day IV or PO, in divided doses every 6 hours (in adults), and 50-75 mg/kg/day IV or PO, in divided doses every 6 hours (in children and infants). In vitro concentrations of 0.1-20 µg/ml of C are generally effective against susceptible strains. Since hematologic toxicity (resulting from C therapy)1-3 can be dose-related, peak serum concentrations above 25 µg/ml are discouraged avoiding its repetitive course and limiting duration of therapy less than 2 to 3 weeks. C is metabolized in the liver by hepatic glucouronyl transferase to the inactive glucuronide, and excreted in the urine, 5-30% following IV dosage; while small amounts are excreted unchanged in the bile and feces following oral administration. The plasma half-life for C is 1.5-4.1 hours in adults with normal renal and hepatic function. Since its introduction in 1948,4 C has been the treatment of choice for TF. Although there were sporadic reports of resistance, the effectiveness of C remained satisfactory until 1989, when there was rapid emergence and spread of multi drug-resistant (MDR) Salmonella enterica serovar Typhi (resistant to ampicillin, C, and trimethoprim-sulfamethoxazole) in several parts of India.5-8 This phenomenon led to the replacement of C by ciprofloxacin (Ci) in the treatment of S. enterica serovar Typhi infection.9 Discontinuation of C therapy is expected to relieve the selection pressure paving the way for re-emergence of S. enterica serovar Typhi isolates sensitive to C.10 But the widespread and injudicious use of Ci, it's reduced activity against S. enterica serovar Typhi infection has been reported.11 C susceptibility test following disk diffusion is not enough for its re-selection in the treatment of TF,12 and therefore, it is imperative to compare the minimum inhibitory concentration values (MICs) of C for the sensitive isolates with C MICs for the resistant isolates. The present study has been undertaken to evaluate the efficacy of C by the determination of MIC values for S. enterica serovar Typhi isolates (1991-2003) for its reintroduction in the treatment of typhoid fever. MATERIAL AND METHODS Strains A total of 464 S. enterica serovar Typhi isolates, which were obtained from blood samples of suspected enteric fever patients (Kolkata and its suburbs) attending Calcutta School of Tropical Medicine for treatment during 1991 and 2003, were used in this study. Such set of samples was used in the present study in order to assess the in vitro efficacy of a valuable antityphoid antibiotic C for its reconsideration in the treatment of Ci-resistant TF. Escherichia coli strain ATCC 25922 was used as the control. Media and antibiotics Mueller-Hinton broth and Mueller-Hinton agar (Hi-Media, Bombay, India) were used for the present study. For disc diffusion susceptibility test different antibiotic discs (Hi-Media, Bombay, India) used in the study were C (30 µg/disc), ampicillin (A; 10 µg/disc), cotrimoxazole (Co; 25 µg/disc), Ci (5 µg/disc), nalidixic acid (Nx; 30 µg/disc), ceftriaxone (Cf; 30 mg/disc) and cefotaxime (Ct; 30 mg/disc). For performing MICs, C, A, Nx, Cf and Ct were obtained from Sigma Chemicals, St. Louis, USA; Ci, Co (sulphamethoxazole, Sm + trimethoprim,Tm) from Hi-Media Laboratory Limited, Mumbai, India. Inoculum preparation Inoculum was prepared from overnight grown broth culture, which was first matched with 0.5 MacFarland standard and then adjusted to approximately 104 CFU/spot (for the determination of MICs) by colony count method. The disc diffusion susceptibility test utilized an inoculum equivalent to 0.5 MacFarland turbidity standard planted on the agar plate. Disc diffusion susceptibility test Disc diffusion susceptibility test13 was performed following the guidelines of the National Committee for Clinical Laboratory Standards (NCCLS) with C for the S. enterica serovar Typhi isolates obtained during 1991-2003; in addition A, Co, Nx, Ci, Cf and Ct were used for the isolates of 2002 and 2003. The inoculated agar plates containing the proper antibiotic disc(s) were incubated for 24h at 370C, and zone diameter obtained around the antibiotic discs were measured. Determination of MICs MICs were determined by the agar dilution method14 according to the criteria of the NCCLS. The concentrations of antibiotics (µg/ml) used were C (0.05-6000) for the isolates obtained during 1991-2003, and A (0.5-2500), Co (0.25-200), Nx (16-512), Ci (0.125-2), Cf and Ct (0.0125-2) for the isolates of 2002 and 2003. Statistical analysis The c2 test with Yates correction was employed to compare and assess yearwise significance in the increase or decrease of C sensitivity of S. enterica serovar Typhi strains isolated during 1991-2003. RESULTS Figure 1 shows the disc diffusion test results for S. enterica serovar Typhi isolates (1991-2001). In 1991, all isolates were found to be resistant (100%), while decreasing frequency of resistance was noticed in the following four years. All isolates from 1996-1999 and 2001 were C-sensitive. In our study 21% isolates of 2000 were resistant. MICs of C ranged between 0.10 and 5 µg/ml for sensitive isolates, while the resistant isolates showed C MICs 150-5000 µg/ml (Table 1). Typhi strains isolated during 2002 and 2003 is summarised, according to the criteria of NCCLS, in Table 2. C susceptibilities for the isolates were 85% and 91%, respectively during 2002 and 2003. All strains were Nx-resistant (MICs 32-256 µg/ml), indicating the reduced susceptibility to Ci (MICs 0.5-1.25 µg/ml) for the isolates (Figure 2). However, all the isolates were sensitive to Ci, by disk diffusion, according to the criteria suggested by the NCCLS. The isolates showed 100% susceptibility to the third-generation cephalosporins (Cf and Ct), but with increased MICs: 0.05-0.5 µg/ml for Cf, and .025-0.5 µg/ml for Ct. A statistical analysis comparing the differences in sensitivity to C of the isolates (1991-2003) is shown in Table 3. The remarkable increase in C sensitivity of S. enterica serovar Typhi isolates observed when compared between the years 1991 and 1992, 1994 and 1995, and 2000 and 2001. DISCUSSION Since 1990, replacement of C by Ci as the drug of choice for TF has been in practice in India.9 Rampant use of Ci, not only for TF but for other infections too, gradually led to increased MICs of S. enterica serovar Typhi to Ci, threatening its therapeutic efficacy.11 On the contrary, withdrawal of selection pressure resulted in the re-emergence of C susceptible S. enterica serovar Typhi isolates, with very low MICs (0.10-5 µg/ml), as is evident from this investigation (Table 1 & 2). Comparison of the strains isolated between 1991 and 2003 revealed interesting fluctuations in susceptibility to C. For instance, there was a striking and abrupt emergence of C-sensitive S. enterica serovar Typhi isolates from 1991 to 1992. The most interesting observation in this study was the progressive increase in the emergence of C-sensitive isolates up to 1999. However, there was reemergence of C-resistant isolates in between the years 2000 and 2003: 27% (in 2000), 15% (in 2002) and 9% (2003). The use of C against the infection of many other enteric bacteria, the strains remain resistant to the drug, and play role as the reservoir of plasmid encoding multiple drug (including C) resistance. Datta et al15 reported the acquisition of R-plasmid by S. enterica serovar Typhi, in the bowel of man, from other enteric bacteria. In our earlier study, we reported the acquisition of R-factor by S. enterica serovar Typhi from MDR E. coli isolates from urinary tract infection cases.16 Furthermore, due to several treatment failures with Ci (manuscript under revision in IJAA, Pal et al) and ofloxacin17 during and after 1995-1996, C, in addition to the third-generation cephalosporins like Cf, was tried in typhoid fever. This selective pressure of antibiotic may be the cause of acquisition of R-plasmid by S. enterica serovar Typhi isolates in the year 200016 and again in 2002 and 2003, which in turn caused C-resistant strains to emerge. It has been reported in our earlier study that in S. enterica serovar Typhi (1991-2001) resistance to C, A, Co and tetracycline is mediated by R-factor, and that it was unstable in S. enterica serovar Typhi16 Thus, high level of C MICs, in resistant isolates, is determined by the acquisition of R-plasmid under selective pressure. In contrast, loss of R-plasmid causes emergence of C-sensitive strains showing very low MICs. Possibly, due to the above fact the wide range of C MICs (0.1-5000 µg/ml) was noticed among the S. enterica serovar Typhi isolates used in the present study. The high degree of C susceptibility to S. enterica serovar Typhi isolates has also been reported very recently from many other parts of India. Sood et al10 reported C sensitivity among 71.9-91.6% isolates during 1994-1998. Bhattacharya and Das18 isolated S. enterica serovar Typhi strains from Orissa of which 87.46% were C- sensitive. Chande et al19 reported C sensitivity in 74.5% S. enterica serovar Typhi isolates from Nagpur with MICs of £ 4 µg/ml. Kumar et al20 reported from Ludhiana that there was an increase of C susceptibility from 43% (1995) to 93% (1999) among S. enterica serovar Typhi strains.Goutam et al12 reported from Rohtak (Haryana) about the reemergence of C sensitivity in 90% S. enterica serovar Typhi isolates by MIC determination. Rodrigues and Mehta21 reported a decrease in occurrence of C resistance in S. enterica serovar Typhi, and they suggested using C, along with the third-generation cephalosporins, in typhoid fever due to Ci-resistant S. enterica serovar Typhi infection. Clinical cure without complications or relapse in 19 patients (83%), treated with C has been reported from Nepal.22 The significant decrease in isolation of C-resistant S. enterica serovar Typhi strains in Bangladesh suggested cheaper and effective first-line antibiotic C as drug of choice for the treatment of typhoid fever.23 Conversely, the use of C is limited because of its toxicity1,2: "aplastic anemia" (which is very rare but can occur after either oral or intravenous administration), "gray baby syndrome", which can be eliminated, and "bone marrow suppression", which can be minimized by using C at the recommended doses and monitoring levels. Furthermore, treatment with C has reduced TF mortality from approximately 20% to 1% and duration of fever from 14-28 days to 3-5 days,1,24 and increased use of C has not resulted in frequent reports of toxicity in the last few decades. Thus, C remains an important inpatient antibiotic that can be invaluable for treating certain life-threatening infections including TF, particularly when the causative organisms are resistant to other antibiotics. It has been suggested that resistance to Nx may be an indicator of low-level resistance to Ci among S. enterica serovar Typhi isolates.25 In the present study all 43 isolates of 2002 and 2003 were Nx-resistant, and Nx resistance wasassociated with the decreased susceptibility to Ci (MICs 0.5-1.25 µg/ml) for the isolates. Nx resistance in association with decreased susceptibility to Ci in S. enterica serovar Typhi is now endemic in different parts of the world including India,26 constituting a threat to global health. In response to the development of Ci resistance among MDR S. enterica serovar Typhi, a number of studies have investigated the efficacies of newer compounds including expanded-spectrum cephalosporins.27,28 Specifically, Cf has been very successful, with low rates of fever relapse, but this agent, like other expanded-spectrum cephalosporins, including Ct and ceftazidime, is hindered by its expense and the need for parenteral administration.29 In the present study, treatment of TF with the third-generation cephalosporins (Cf and Ct) has been suggested based on their in vitro activity against S. enterica serovar Typhi isolates (MICs 0.025-0.5 µg/ml). Presently, treatment failure of MDRTF with cephalosporins have been reported29 and in some cases30 with high-level resistance to Cf (MIC 64 µg/ml) in S. enterica serovar Typhi. Thus the situation demands fresh consideration for the use of C in TF instead of using newer quinolones or cephalosporins of third-generation to prevent the emergence of resistance to these drugs. REFERENCES
Copyright by The Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04003t2.jpg] [ms04003f1.jpg] [ms04003f2.jpg] [ms04003t1.jpg] [ms04003t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}