 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Science Vol. 58 No. 2, February 2004 , pp. 47-53 Original Contributions Outbreak of measles amongst vaccinated children in a slum of Chandigarh Munesh K Sharma, Vikas Bhatia, H M Swami MBBS, MD, PGDHM, Senior Lecturer-cum-Epidemiologist; MBBS, MD, Senior Lecturer; MBBS, MD, FIAPSM, Prof. & Head; Department of Community Medicine, Govt. Medical College, College Building, Sector 32-A, Chandigarh - 160030, India.
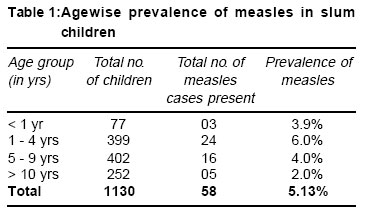
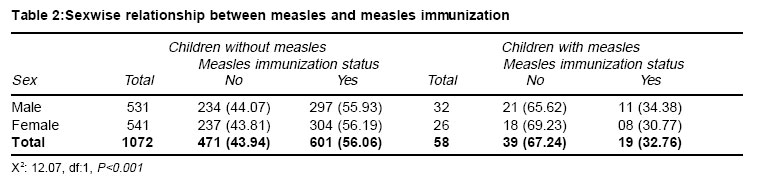
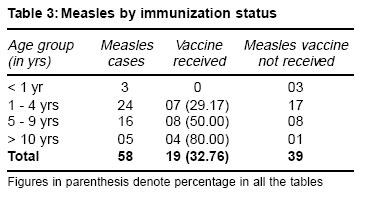
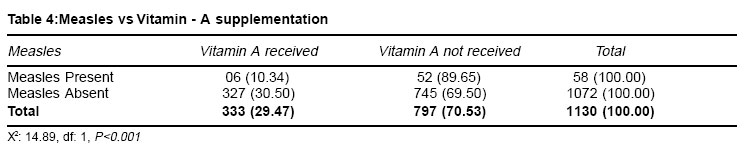
Accepted Date: 25-02-2004 Code Number: ms04007 ABSTRACT Background: An outbreak of measles was reported from a slum, UT, Chandigarh in April 2003. Similar outbreak was also reported in less than three years from the same and adjoining areas. The present study was conducted to investigate and assess various epidemiological features associated with measles outbreak. Material and Methods: Three cases of measles were admitted in Deptt. of Paediatrics, Govt. Medical College & Hospital, Chandigarh and were reported to the Deptt. of Community Medicine for an outbreak investigation. A trained team investigated the slum having a population of 25,000 and studied various features associated with epidemic between the period of April 22 to May 10, 2003. Results: The study covered 484 houses having 1130 children. Among the children who developed measles 32.76% were vaccinated ones. In them attack rate was 3%. Attack rate in vaccinated children went on increasing as age increased. An overall attack rate of 5.13% (Peak incidence 6% in 1-4 years age group) was recorded. Among measles cases, one-fifth had post measles complications. As much as 32.76% children with measles had received measles vaccination in the past. Therefore something more than immunization by single dose of vaccine is required. Measles was reported to be higher amongst the children without Vitamin A supplementation (P<0.001). Conclusion: There is need to store vaccine properly and to strengthen routine immunization coverage, Vitamin A supplementation and health infrastructure in underprivileged population. Serological studies among vaccinated children against measles should be undertaken to explore the possibility of second dose of measles in older children. KEY WORDS: Measles, Epidemic, Immunization, Vitamin A supplementation. INTRODUCTION Measles is one of the frequently occurring infectious diseases among children. Its incidence varies from 58 percent in epidemics to 10-15 percent without it in paediatrics age group.1,2 Malnutrition, poverty, overcrowding, poor hygiene, vit. A deficiency, improper immunization and decreased immunity are the factors associated with this disease. WHO estimates that almost 1 million measles-related deaths occur each year, the majority (85%) in Africa and Asia.3 The burden from mealses in industrialized countries is not insignificant.4 During a resurgence of measles in the United State between 1989 and 1991, more that 11000 patients were hospitalized and 123 persons died.5 Measles ends in complications in various proportions. In 2001 the total number of confirmed cases in the Americas reached a record low of 541 cases, 99% reduction compared with 1990. Siliguri epidemic killed more than 20 persons in the year 2001 including doctors & nurses. Over a period of time in the last decade a declined trend in immunization coverage has been observed in most of the states in India. By the end of 1990-91, the reported coverage for measles was 91% which declined to 84% in 1998-99.6 Therefore the present study was conducted in slum population of Chandigarh to investigate and assess various epidemiological features associated with measles outbreak and occurrence of measles among vaccinated children. MATERIAL and METHODS Under the surveillance reporting system established by the Department of Community Medicine, Govt. Medical College, Chandigarh all the defined cases of infectious diseases diagnosed in various clinical departments of the hospital are reported here. Three cases of measles were admitted in the Department of Paediatrics, Govt. Medical College & Hospital, Chandigarh and reported to the department. The exact address as of these cases were procured and a team comprising of doctors, medical social workers and interns were sent to the affected area in slum (Colony No. 5) for outbreak investigation. The team was trained on various aspects of investigations in order to collect the uniform information. Colony No. 5 is one of the largest slum in Chandigarh with a population of about 25,000 and has migrants from the states of Uttar Pradesh, Bihar, Jharkhand etc. This slum is located at about 2 Kms from the Govt. Medical College & hospital. A format based on instructions given in Director General of Health Services, Govt. of India, National Institute of Communicable Diseases, Delhi's manual on epidemiological surveillance procedures for selected diseases 19847 was developed comprising of selected information on measles outbreak investigation. Only the clinical & operational definition of measles case was considered firstly because index case was already evaluated by experts from paediatric department and secondly facility for laboratory diagnosis is not available in Govt. Medical College & Hospital, Chandigarh. If a child upto the age of 14 years, had suffered from fever, maculopapular rash with cough, running nose/ watering from eyes with or without redness (Comparable to the ones admitted in Paediatric Ward) he/she was diagnosed as a case of measles. This definition was considered as diagnostic of measles and was adhered to throughout the study. The clinical presentation, nature of rash and similarity in presentation of cases in slum index case measles from the same area having being admitted in tertiary hospital and diagnosis settled by pediatricians are clearly strong enough to label them as measles cases. A period of 90 days preceding April 20, 2003 was considered for inclusion of children in the outbreak. Area having reported measles cases was extensively covered by making house to house visit and enquiries about measles cases were made from the mothers or responsible persons. Information was collected on family history regarding measles in subjects, measles immunization status which was assessed by checking the immunization cards and history, post-measles complication covering diarrhoea, otitis media, pneumonia, encephalitis etc. Only 669 cards could be traced. History of immunization was asked from mother. Interestingly measles immunization history either in affirmative or in negative was available for all children. The records recall method and in depth discussion about immunization history helped in noting down the measles vaccination status. Two, three or even more visits were made in household where partial information was available in first visit specially to meet mother for eliciting history of immunization. Vitamin A supplementation was considered if at least one dose of Vitamin A solution was taken by a child. The study was conducted between the period of April 20, 2003 and May 10, 2003 which covered children upto the age of 14 years in the affected area of the slum. The data was analysed according to age, sex, measles immunization, Vitamin A supplementation and post-measles complications. RESULTS The study on outbreak of measles was conducted in one of the largest slum of Chandigarh covering 484 households and 1130 children. The first case / index case was recorded on 22nd Feb. 2003, through 3 cases of measles were admitted in department of Paediatrics in Mid-April 2003, and the last case of measles was detected on May 11, 2003. With further follow-up visits no other case could be detected. It can be seen from Table 1 that among 1130 children, 58 children suffered from measles i.e. overall attack rate of 5.13%. The peak incidence of 6.0% was recorded in the age group of 1-4 years. Five cases were also observed in the children beyond 10 year of age. Measles complications were present in 12 (20.03%) of cases; with diarrhoea in 4, pneumonia in 3, otitis media in 3 and encephalitis in 2. Appropriate management was done as needed in these cases. Team which included medical officers and first author, carried with it ORS packets, Vitamin A, antibiotics etc. and managed 28 cases. Rest 30 patients were taken to Urban Health Training Centre-44, Chandigarh (which is situated just 0.5km from the study area) by college mini bus. Out of these both cases of encephalitis and one case of otitis media were further taken to Govt. Medical College & Hospital, Sector-32, Chandigarh for proper management. On comparing children suffering from measles and not suffering from measles in relation to immunization status, it was observed that 67.24% children were not immunized in the group where measles was reported in comparison to 43.94% in the group where measles was not reported. More cases of measles were observed in the group where immunization coverage was lower. Attack rate in vaccinated children was 3% and in unvaccinated ones it was 7.5%. Relationship between measles cases and vaccination was found to be highly significant (P<0.001). The trend was similar for both the sexes Table 2. Table 3 depicts that out of all (58) measles children, 19 (32.76%) were immunized. The disease attached only un-immunized children in the infancy. The proportion of children attached by measles even after immunization went on increasing with the increase in age. Thus in the age group of 10-14 years almost 80% children with measles were those who received immunization. This reflects decreased efficacy of vaccine with increase in the age which in turn can be due to several factors. Among 58 measles cases, the Vitamin A supplementation was recorded lower i.e. 10.34% in comparison to the 1072 children without measles where 30.5% had received Vitamin A solution. (Table 4) Overall only 29.47% of the study children had received Vitamin A supplementation. A highly significant relationship (P<0.001) was observed between Vitamin A supplementation and measles cases. DISCUSSION The incidence of measles in the present study was less than the other studies which may well be because its incidence in the present study was observed in the age group of 0-15 years as against many studies which depicts its incidence in age group < 10 years.8-12 Peru study however, reported attack rate of 29.26% in the same age group.13 The incidence was however comparable in a similar epidemic of 2001from the same area of Chandigarh.14 Occurrence of two epidemics within a span of less than 3 years in the same population of slum is basically because a large number of children have migrated from Uttar Pradesh and Bihar-the states having poor health indicators including poor immunization of preschool children. This adds to the pool of susceptible children. The lack of hygiene, lower immunization coverage, overcrowding and high illiteracy in the underprivileged population increased the risk of measles transmission. Further the measles immunization coverage in this study was only 54.87% in the age group of 0-14 years and 55.09% in the age group of 9 months to 3 years. The male & female children were immunized to almost equal extent. The immunization coverage was found to be less than national coverage15 but corresponded to the immunization coverage in a study conducted on children of BIMARU states.16 It is expected as most of the children in the present study area were from the states of Uttar Pradesh & Bihar. One third of the measles cases were from amongst the vaccinated children in the present study. In infancy, disease attacked only un-immunized children but as the age advanced even immunized children suffered from measles. In the age group of 1-4 years, 29.17 % immunized children suffered, in the age group of 5-10 years 50% and in older children of age group 10-14 years almost 80% suffered from measles inspite of immunization. This suggests waning of immunity with age which can be due to the use of poorly stored vaccine at the place of these childrens' vaccination. However, effect of exposure to ultra violet radiation to wane immunity as observed by Prof. Mary Norval cannot be ruled out17 can not be ruled out. There appears to be a need for better storage of vaccines and the need of second dose of measles vaccine at the age of school entry may be a point of further study. Many developed countries like Finland, Hungry, United States, Canada, Oman, United Kingdom had eliminated measles by 2 doses schedule.18 The measles related complications in the present study were observed in one-fifth of cases. This rate is less than the rate of measles related complications reported by other workers19,12,14 and more than global average.20 In 12.07 percent of measles cases with complications, diarrhoea was the commonest problem. This is very much possible as noted by May CJ Rudoff.19 In the present study maximum cases (41.38%) of measles were in the age group of 1 to 5 years as noted by others.14,21 Peak attack rate in the same age group was also reported 3 years back in the same area.14 Further Snidack DH et al reported an attack rate of 42.6 percent in the age group of 16-30 years and 16.7 percent in the age group of 31-40 years.13 Similarly high incidence of 23.5 % in the age group of 10-14 years has been noted by others.22 These reports point out towards age shift of measles attack. No measles related death was reported in present outbreak. Similar findings have been reported by others workers.11,14 Low attack rates, no mortality and fewer complications reflected the mild nature of the outbreak which in turn was because of better awareness and availability of health services. In fact the hospitalized cases were the initiating factor to start further investigation. Protective effect of vitamin A on child in preventing measles is as expected because vitamin A deficiency is a form of malnutrition and measles in an infection. An association between vitamin A deficiency and measles occurrence has been observed by Shears et al23 and others.24 CONCLUSION From the present study it may be concluded that there is a need to re-conduct epidemiological & serological studies to find out the magnitude of sero-conversion amongst vaccinated, and non-vaccinated children in different parts of our country as has been done in the past. Depending upon the results, before considering the possibility of second dose of measles in older children an emphasis must be on an urgent need to strengthen universal coverage by properly stored potent measles vaccine by at least one dose. Maintenance of cold chain is of paramount importance. REFERENCES
Copyright by The Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04007t4.jpg] [ms04007t2.jpg] [ms04007t3.jpg] [ms04007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}