 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Science Vol. 58 No. 2, February 2004 , pp. 54-61 Sublingual misoprostol before first trimester abortion: A comparative study using two dose regimens N Vimala, S Mittal, S Kumar M.D., Research Officer; M.D., Prof. & Head; M.D, Professor, Department of Obstetrics & Gynaecology, AIIMS, New Delhi, India.
Accepted Date: 25-02-2004 Code Number: ms04008 ABSTRACT Various methods have been described for preoperative cervical priming prior to vacuum aspiration (VA) in first trimester pregnancy termination, to facilitate cervical dilatation and shorten the abortion procedure. Recently misoprostol a prostaglandin E1 analogue has been shown to be effective in facilitating cervical dilatation prior to VA. Misoprostol offers several advantages over the other prostagland in analogues including stability at room temparature, ease of administration and minimal side effects. Objective: To determine the optimal dosage and dosing interval for the use of misoprostol administered sublingually for pre-abortion cervical dilatation. Setting & Design: This was a prospective randomised study conducted at Comprehensive Rural Health Project, Ballabgarh the rural health centre under Centre for Community Medicine, AIIMS, New Delhi. Material and Methods: One hundred and twenty pregnant women between 6-11 weeks of gestation opting for voluntary medical termination of pregnancy were (MTP) randomly allocated to either 200 µg or the 400 µg misoprostol group. Vacuum aspiration was performed either two or three hours after administration of sublingual misoprostol. Using Hegar's dilators, degree of cervical dilatation before vacuum aspiration was measured. Other parameters assessed included the amount of additional dilatation required, intra-operative blood loss and associated side effects. Statistics: Statistical analysis was conducted using chisquare, the student's t and the Mann-Whitney U tests to examine the difference between the two groups. Results: In the 200 µg misoprostol group 33% achieved a dilatation of > 8 mm compared with 71% of women in the 400 µg misoprostol group. The odds ratio was 95.8 (95% CI 10.2-842.9) for 400 µg misoprostol for successful preoperative cervical dilatation of > 8 mm. The mean baseline cervical dilatation for 400 µg and 200 µg misoprostol was 8.2 mm and 6.0 mm respectively (P<0.001). The use of 400 µg misoprostol with an evacuation interval of two hours appears to be the optimal dosage and evacuation interval. Increasing the time interval beyond two hours did not confer any additional advantage on the rate of successful cervical dilatation but was instead associated with an increased incidence of side effects such as preoperative vaginal bleeding, abdominal pain and shivering. Conclusion: Our study has shown that Sublingual administration of 400 µg of misoprostol at least two hours before procedure is effective for preoperative cervical dilatation before vacuum aspiration in first trimester pregnancy termination. There is no additional advantages of increasing the dosing interval upto three hours. KEY WORDS: Pre abortion cervical priming, Misoprostol, First trimester pregnancy. Introduction Cervical priming prior to first trimester surgical abortion facilitates the procedure and reduces the risk of cervical injury and uterine perforation1,2 that are often associated with mechanical cervical dilatation of nulli parous cervix. Pharmacological agents commonly used for this purpose include laminaria tents and prostaglandins. Although prostaglandin analogues like gemeprost, produce more effective cervical ripening and are more convenient to administer than laminaria tents3 they are expensive, require cool storage and associated with several adverse effects like nausea, vomiting, abdominal pain and diarrhea.4 The ideal cervical priming agent should be effective and easy to administer, with a low incidence of side effects. Misoprostol a synthetic prostaglandin E1 analogue used for the prevention and treatment of peptic ulcer disease has been studied for medical abortion,5 for induction of labor at term6 and for cervical priming prior to surgical abortion.7 It has the advantages of easy availability, ease of administration, lower cost, stability at room temperature and fewer systemic side effects. Misoprostol has been administered orally, buccally sublingually, rectally and vaginally, the vaginal route has been shown to be more effective for preabortion cervical ripening in comparative studies of oral and vaginal administration.7,8 Recent studies have considered the effectiveness, safety and patient acceptance of sublingually administered misoprostol. A pharmacokinetic study9 by Tang et al showed that the systemic bioavailability of sublingually administered misoprostol is significantly much higher than that after vaginal administration. In a previous study,10 we have shown that misoprostol administered sublingually in a dose of 400 µg two hours prior to surgical abortion is effective in facilitating cervical dilatation and was associated with side effects including abdominal pain, shivering, nausea, vomitings and preoperative vaginal bleeding. In present study we wished to investigate the sublingual route further and compare two doses regimens in an effort to minimize the side effects while maintaining the efficacy. The aim of this study was to determine the optimal dosage and timing for the sublingual use of misoprostol for preoperative cervical dilatation in women undergoing surgical abortion for first trimester pregnancy. The comparison was made between 200 µg and 400 µg dosage of misoprostol.
Material and Methods
This study was conducted at Comprehensive Rural Health Service Project Ballabgarh. This is a secondary referral teaching hospital and rural field practice area of AIIMS hospital, New Delhi.
One hundred and twenty pregnant women between 6-11 weeks of gestation opting for termination of first trimester pregnancy between 1st Oct. 2002 30th Jan. 2003 were included in this study. The study was approved by local research ethics committee. An informed written consent was obtained from all the women willing to participate in the study. Women with heart disease, asthma, known allergy to prostaglandins, multiple pregnancies, and scarred uterus and were excluded. Gestation was assessed by the menstrual history and clinical examination. Ultrasound was performed, in six women for conformation of gestational age, of them 4 were conceived during lactational amenorrhoea, one had previous history of molar pregnancy and in one women uterine size appeared less than the period of amenorrhoea as she had irregular menstrual cycles. Women were randomized to either 200 µg or 400 µg misoprostol dosage groups. Randomization was achieved by the opening of sequentially numbered sealed envelopes prepared using random number tables. The women were admitted on the morning of the procedure and the appropriate dose of misoprostol was administered sublingually by a doctor who was not one of the surgeons assessing the treatment outcome. The vital signs including blood pressure, pulse rate, temperature and the occurrence of side effects such as abdominal pain, vaginal bleeding, nausea, vomiting, shivering, fever and diarrhoea before vacuum aspiration were recorded. The severity of abdominal pain experienced by the women was assessed using a three-point scale of 1 (no pain) to 3 (severe pain requiring analgesics). Similarly, preoperative vaginal bleeding was measured on a scale of 1 to 3. (1: Spotting or minimal bleeding, 2 : bleeding like menstrual flow, 3: heavy bleeding with clots).
Women from each of the two groups were further randomly allocated to two subgroups and the vacuum aspiration was performed under intravenous analgesia (Pentazocin 30 mg + diazepam 10 mg) at either two or three hours after the insertion of misoprostol tablets. The vacuum aspiration was performed in all the women by the lead investigator (V.N.) to reduce individual variation. The randomization schedule was unknown to the surgeon performing VA and measuring the outcomes but women and the doctor administering the drug were aware of treatment allocated. The degree of cervical dilatation before vacuum aspiration was used as a primary outcome measure and it was measured by passing the Hegar's dilators in descending order starting with Hegar's no: 12. The size of the largest Hegar's dilator that could be passed into the cervical os without resistance was recorded as the cervical dilatation achieved. If the cervix had dilated to > 8 mm no further dilatation was performed and the pregnancy was evacuated with a number 8 Karman's cannula. Secondary outcome measures that were assessed intraoperatvely included the amount of further dilatation required to permit passage of the suction cannula, intraoperative blood loss. Intraoperative blood loss was taken as the volume of the total uterine aspirate after shivering away the products of conception measured with a measuring cylinder. Following the procedure the women were kept in hospital for two hours before discharge and they all attended a follow up visit at 6-8 weeks.
The sample size was calculated on the basis of the effects on cervical dilatation seen in previous studies.10,14-18 A two group x2 test with a 0.05 two sided significance and a power of 95% the sample size in each group should be 47. Assuming 20% default at follow-up the number chosen was 60 in each group. Statistical analysis was performed using Chisquare test the student's `t' test, Fisher's exact test and the Mann-Whitney U test.
Results
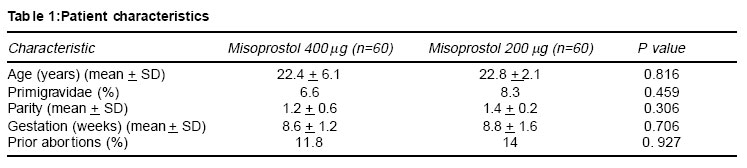
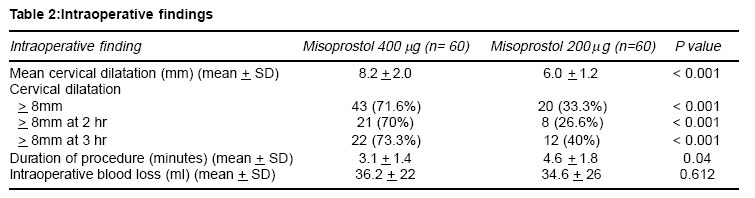
The two treatment groups were similar in relation to maternal age, parity and gestational age (Table 1). None of the women aborted during the interval between misoprostol administration and the scheduled time of evacuation of the uterus. The mean cervical dilatation for 400 µg and 200 µg misoprostol was 8.2 m and 6.0 mm respectively (P<0.001). Twenty women (33%) in 200 µg misoprostol group achieved a dilatation of > 8 mm or more, compared to 43 women (71.6%) who had received 400 µg misoprostol. The odds ratio was 95.8 (95% CI 10.2 842.9) for 400 µg misoprostol for successful preoperative cervical dilatation of > 8 mm (Table 2). High success rate with preoperative cervical dilatation was achieved using 400 µg misoprostol at both two hours (70%) and three hours (73%) but with 200 µg misoprostol group only eight women (26%) achieved cervical dilatation at two hours interval, compared 12 women (40%) who had a time interval of three hours. The mean intraoperative blood loss was found to be similar in both the groups (P=0.612), (Table 2).
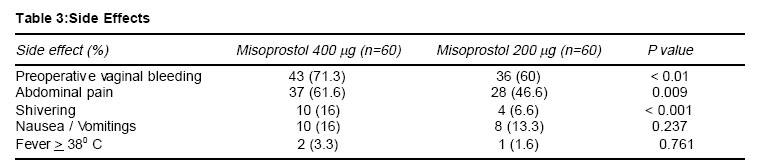
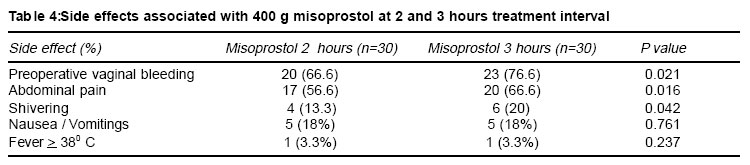
More women experienced vaginal bleeding, abdominal pain and shivering, in the 400 µg misoprostol group compared with the 200 µg misoprostol group (Table 3) and this difference was statistically significant (P<0.05). However, these symptoms were mild and required no additional treatment. In the 400 µg misoprostol group; it was observed that some side effects were more frequent at three hours as compared with two hours (Table 4). The incidence of preoperative vaginal bleeding, abdominal pain and shivering were significantly higher at three hours (P<0.05). No major side effects such as excessive hemorrhage (>500 ml), uterine perforation or incomplete abortion, were seen in either group. The average time taken for vacuum aspiration was 3.1 + 1.4 minutes in the 400 µg misoprostol group and 4.6 + 1.8 minutes in the 200 µg group (P=0.04). At the follow up visit at 6-8 weeks all women had resumed their menses and none had reported any side effects.
Discussion
The unmet need for safe pregnancy interruption in many countries makes it highly desirable to find simple methods to effect a quick, hygienic, and uncomplicated uterine evacuation. Mechanical dilatation of cervix followed by vacuum aspiration is a commonly used method for termination of first trimester pregnancy. Forced mechanical dilatation of cervix may result in cervical laceration, uterine perforation and hemorrhage.11 Increased incidence of spontaneous abortions and in-competence of cervix in subsequent pregnancies have also been suggested to be related to forced dilatation.11 The pharmacological agents often used are hydrophilic intra-cervical tents12 and prostaglandins. Laminaria tents are inexpensive but they require trained personnel for insertion, complications such as displacement of tent inside the uterus and perforation of uterus may occur12,13 prostaglandin analogues such as gemeprost have also been shown to be effective for cervical priming. However these are expensive, unstable and requires refrigeration for storage.7,8 The low cost and ease of storage of misoprostol makes it an attractive alternative to other prostaglandins for preoperative cervical dilatation before pregnancy termination by vacuum aspiration. Oral as well as intravaginal administration was studied in concentrations of 200 to 600 mg of misoprostol used 30 minutes to 12 hours before the surgical procedure.14-19 All the studies concluded misoprostol to be significantly more effective than placebo and at least as effective as other prostaglandin analogues such as gemeprost and sulprostone regarding loss of blood, duration of surgery, baseline dilatation.
However, majority of comparative studies have found that vaginal administration of misoprostol is more effective than oral administration. This was supported by a pharmacokinetic study showing that the systemic bioavailability, as demonstrated by the area under the curve, after vaginal misoprostol was three times higher than that after oral misoprostol.20 There has been evidence showing that absorption through vaginal route is inconsistent and in addition women preferred to misoprostol tablets by mouth in order to avoid uncomfortable vaginal examination.20,21 Therefore, the oral and the vaginal routes of administration may not be the optimal way of administering misoprostol for cervical priming. Recently sublingual administration of misoprostol is being evaluated as an alternative to oral and vaginal administration for medical abortions, and cervical ripening.23 These initial studies have found it to be a every effective and convenient route of administration.
Two previous studies have evaluated the use of sublingual misoprostol as preabortion cervical priming agent and have shown that it is more effective than placebo in facilitating cervical dilatation and it's usage, significantly reduced pain perception, intraoperative blood loss and time duration of surgery.24
The success of cervical dilatation associated with the use of misoprostol increases with both dosage and evacuation time interval.25 Fong et al compared two doses of vaginal misoprostol (400 µg vs 200 µg) administered either at 3 or 4 hours interval and found that vaginal administration of 400 µg of misoprostol at 3 hours intervals was optimal for preoperative cervical dilation before vacuum aspiration.25 The results of our study demonstrates that the use of 400 µg sublingual misoprostol was significantly more effective than 200 µg in achieving a preoperative cervical dilatation of > 8 mm (odd ratio of 95.8).
Increasing the time interval beyond two hours did not appear to offer any additional advantage on the rate of successful cervical dilatation, instead the incidence of side effects such as shivering, abdominal pain shivering were significantly increased.
The side effects associated with the use of sublingual misoprostol are similar to that reported in other studies,22,23 with vaginal bleeding, abdominal pain and shivering being the most common side effects reported by the women in our study. Studies in which vaginal misoprostol has been used in doses varying form 200 µg to 1000 µg over 12 hours prior to abortion14-18 have shown that an increasing dosage and time interval before evacuation is associated with an increase in the side effects. Absence of blinding of all investigators and use of subjective measures to assess the cervical dilatation are potential source of bias in the present study.
From our study it appears that the use of 400 µg misoprostol sublingually with an evacuation interval of two hours is effective in facilitating preabortion cervical priming prior to termination of first trimester pregnancy and there is no additional advantage of increasing the dosing interval upto three hours. However it needs to be further investigated in larger randomized studies. References
Copyright by The Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04008t1.jpg] [ms04008t4.jpg] [ms04008t3.jpg] [ms04008t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}