 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
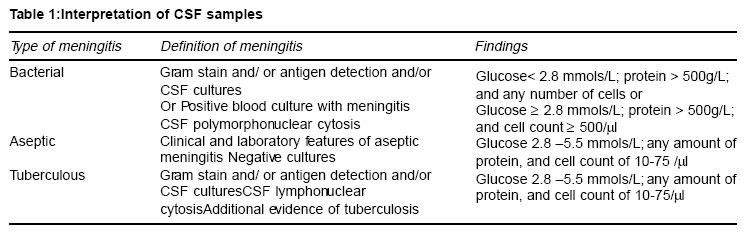
Indian Journal of Medical Science Vol. 58 No. 2, February 2004 , pp. 62-66 Rapid Diagnosis of Meningitis Using Reagent Strips Ramesh C Parmar, Swapna Warke, Poonam Sira, Jaishree R Kamat MD, DCH, FCPS, DNB, MNAMS, FIPC Ex-resident; MD, DCH, Ex-resident; MD, DCH Professor; Department of Pediatrics, Seth G. S. Medical College & K. E. M. Hospital, Parel, Mumbai - 400012, India.
Code Number: ms04009 ABSTRACT Objectives: Identification of causative agent with estimation of cerebrospinal fluid (CSF) glucose, protein, cells is necessary for accurate diagnosis of meningitis. Unfortunately, even these facilities are not available in many areas. Reagent strips that measure glucose and protein in blood and urine can serve this task but have been used with varying results in the past. This study was carried out to evaluate the utility and efficacy of Combur 10 strips in the diagnosis of meningitis. Design, settings and methods: A prospective clinical single blinded study of 63 children suspected to have meningitis undergoing CSF analysis. Each CSF sample was divided in to two and was utilised for reagent strip analysis in addition to standard laboratory evaluation and a correlation analysis were made. Statistical Method used: Results were analysed using standard statistical tests. Accuracy of the reagent strips as a screening tool was established using Godyn's test. Results: The sensitivity, specificity of the reagent strips for the diagnosis of meningitis was 97.14%, 96.42%. The sensitivity, specificity for tuberculous meningitis and bacterial meningitis were 100%, and 96.55%. That for the aseptic meningitis was 70% and 96.55%. Accuracy for the diagnosis of meningitis as a whole, bacterial meningitis, tuberculous meningitis, and aseptic meningitis were 96.78%, 98.2%, 98.27% and 83.0% respectively. Conclusion: Combur10 strips thus can be used for the rapid CSF analysis and screening with good accuracy. In situations where facilities of routine laboratory testing are not available this can be of an immense help. KEY WORDS: Meningitis, rapid diagnosis, reagent strips Introduction Early diagnosis and prompt treatment are the cornerstones of the management of children with meningitis. Identification of the causative agent remains the gold standard for the diagnosis. Unfortunately the positivity rate of gram staining and cultures remain low between 25- 40% as against the rate of 80-85% from the developed world.1,2,3 Given the limitations and non-availability of culture methods, many of the treating physicians have to rely upon the clinical assessment and results of the biochemical and cell analysis of the CSF for making the diagnosis of meningitis and classifying its subtypes (Table - 1). Unfortunately even these facilities are not available in many regions of the world. Reagent strips that measures glucose and protein in blood and urine have been used with varying results to evaluate CSF in the past.4-7 If proven useful it can serve as an important tool in the management of these children. Combur-10 (Boehringer Mannheim) is a 10-patch strip used to test urine for specific gravity, protein, glucose, leukocytes, nitrites, pH, haemoglobin, ketones, bilirubin, and urobilinogen. We used this test strip to measure the CSF protein, glucose and leukocytes with the aim to evaluate the utility of Combur10 urine reagent strips for the diagnosis of meningitis and its subtypes and also to correlate its accuracy with the laboratory method for CSF analysis. MATERIAL AND METHODS This prospective, clinical, single blinded study was conducted in paediatric wards and Paediatric Intensive Care Unit (PICU) of a General Hospital over a period of one year after clearance from Hospital Ethics Committee. 63 samples from children suspected to have meningitis constituted study material. All patients underwent a lumbar puncture following thorough clinical evaluation and fundoscopic examination. Each CSF sample divided in to two parts, which were subsequently utilised for routine diagnostic tests and reagent strip analysis of glucose, protein and leukocyte. All the CSF samples were subjected to routine microbiological evaluation. Neuroimaging was carried out whenever clinically warranted. The reagent strip analysis was carried out immediately after obtaining the sample by one of the investigators (SW) and an independent blinded observer. The technicians performing the analysis in the laboratory was unaware of the results obtained. If adequate CSF was not available, the reagent strip was directly dipped in to the CSF or else the CSF was withdrawn into a pipette and 1-2 drops were poured on the glucose, protein and leukocyte patches. The CSF was washed off after 60 seconds and the colour change was read against the standard provided. The presence of leukocytes was graded as negative, 10-25, 75, and 500/microl; protein as 30, 100 and 500 g/L; and glucose as less than 2.8, 2.8, 5.5 mmols/L. Laboratory values of CSF glucose, protein and leukocytes were plotted against the corresponding value of reagent strip category. Because of the skewed deviation natural log values were used. No direct correlation was posed because the strip data was categorical and the laboratory data was continuous. Instead, midpoints between the dipstick category were taken as cut-points to determine the ranges for each category and the number of laboratory values falling within theses were counted and agreement assessed by the kappa statistics. The results obtained by the strip method for each CSF sample were also given to an additional independent observer, unaware of the clinical and laboratory findings, who was also asked to classify the type of meningitis as per the accepted clinical practice (Table-1). The diagnosis made was then compared with the final diagnosis based on the clinical and laboratory results. The sensitivity, specificity, positive predictive value and the negative predictive values of the reagent strips for the diagnosis of meningitis and its subtypes were calculated. Accuracy of the reagent strips as a screening tool was established using Godyn's test. RESULTS A total of 63 samples were analysed. There were 37 males and 26 females. Majority of patients were between 1-5 years of age (52.38%). The relationship between the dipstick and laboratory values for glucose, protein and cell count is shown in the figure 1 ,2 and 3. The number of laboratory values that fell within the range set by the cutpoints of 1 S.D. were 54 out of 63 (85.71%) for protein, 53 (84.1%) for glucose and 54 (85.71%) for cell counts (kappa 0.78, 0.75, 0.78; p < 0.001). On the basis of laboratory evaluation, supported by the clinical findings (10), and normal (28) categories (Table 1). The laboratory diagnosed a total of 35 cases of meningitis. Of these 34 were diagnosed by the reagent strip. Both the investigator and an unbiased observer diagnosed the 12 cases of bacterial meningitis and 13 cases of tuberculous meningitis. Each of them diagnosed an additional case of bacterial and tuberculosis meningitis spuriously (in same patient). However for the aseptic meningitis there was a discrepancy. The investigator diagnosed 8 cases correctly but had one false positive (normal according to laboratory) and two false negative cases (one was normal and other was diagnosed as tuberculous meningitis by reagent strip). While the observer had one false negative case and one false negative case. The sensitivity, specificity, positive predictive value and the negative predictive values of the reagent strips for the diagnosis of meningitis were 97.14%, 96.42%, 97.14% and 96.42% respectively. The sensitivity, specificity, positive predictive value and the negative predictive values of the reagent strips for the diagnosis of bacterial meningitis were 100%, 96.55%, 92.3% and 100% respectively. The sensitivity, specificity, positive predictive value and the negative predictive values of the reagent strips for the diagnosis of tuberculous meningitis were 100%, 96.55%, 92.14% and 100% respectively. The sensitivity, specificity, positive predictive value and the negative predictive values of the reagent strips for the diagnosis of aseptic meningitis were 70%, 96.55%, 87.5% and 92.5% respectively. Out of the 63 cases in the study, 4 cases (3 cases of aseptic meningitis and 1 normal) did not correlate with the diagnosis by the reagent strip. The misdiagnoses in the 3 cases of aseptic meningitis were bacterial, tuberculous meningitis and normal one each. The fourth one normal by conventional method was diagnosed as a case of aseptic meningitis by the reagent strip. Among all the cases of the bacterial meningitis cultures were positive in only in16% (again suggesting the low positive rate and its limited utility as the sole criteria for diagnosis as in many set ups in the developing world), others were labelled as presumed bacterial meningitis. The organisms identified in the confirmed cases were H. Influenzae and Staph. Aureus. CT scan findings in the cases with tuberculosis meningitis were corroborative in the diagnosis and included basal exudates, hydrocephalus and tuberculomas. A cost analysis revealed that the cost of the screening test could be reduced to $ 0.33 (14.92 rupees) if the strip is reduced to the three patches of interest. DISCUSSION No rapid diagnosis tests exist for the analysis of CSF. Our results show that the rapid diagnosis of meningitis can be made with the Combur-10 reagent strips with a high specificity and sensitivity. This test can help in the making the rapid decision whether to use or withhold antibiotics in patients with meningitis. It is easy to do and would be of particular value in the parts of the world where no laboratory facilities exist and referral at higher centres is not possible. The test strip could be simplified to only the three patches of interest, which will help in cutting down the cost to about Rs. 15.00 per strip. Even in the places where these tests are available the conventional methods require preservation of sample and quick processing at least within 2 hours. Albeit, there is always a waiting period before the results are available. Urine reagent strips may help as a complimentary method in this scenario for guiding the physicians in deciding an opt management till the conventional results are available. The overall sensitivity and specificity in our study was about 97.14% and 96.42% respectively. The sensitivity and specificity were low only in cases of aseptic meningitis, where sensitivity is slightly low up to 70% but specificity is good being 96.55%. To judge the suitability of different reagent strip for reproducibility in CSF analysis Godyn proposed the scoring system of accuracy.8 Score of more than 80 were deemed necessary to indicate the reagent strip method as an acceptable screening procedure. Our accuracy for the diagnosis of meningitis as a whole, bacterial meningitis, tuberculous meningitis, and aseptic meningitis were 96.78%, 98.2%, 98.27% and 83.0% respectively. Hence we conclude that Combur-10 strips can be used for the rapid CSF analysis and screening with good accuracy. Relatively small sample size, absence of positive culture results in majority of the cases were the limitations of this study. Moreover we studied only single specific type of reagent strip and did not compare the result from two different types of reagent strip. Albeit, given the results, low cost of analysis, efficacy, rapid availability of results with the reagent strips, has laid down its future use in rapid CSF analysis in diagnosis of meningitis. REFERENCES
Copyright by The Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04009t1.jpg] [ms04009f1.jpg] [ms04009f3.jpg] [ms04009f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}