 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Science Vol. 58 No. 3, March 2004 , pp. 115-121 EPIDEMIOLOGY BASED ETIOLOGICAL STUDY OF PEDIATRIC CATARACTS IN WESTERN INDIA S R KAID JOHAR, N K SAVALIA, A R VASAVADA, P D GUPTA Iladevi Cataract and IOL Research Centre, Gurukul road, Memnagar,
Ahmedabad - 380052, India.
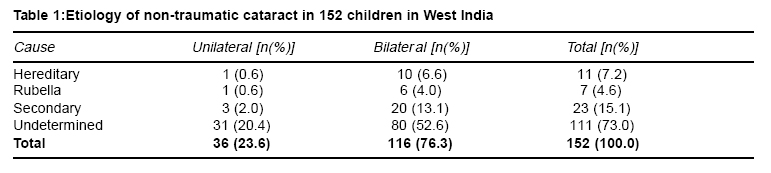
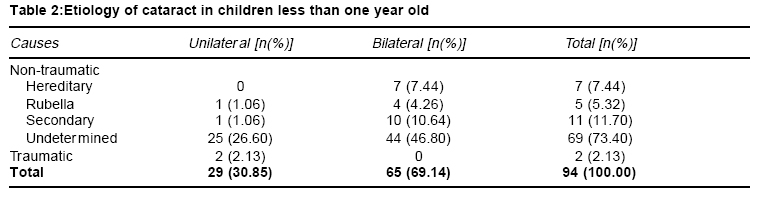
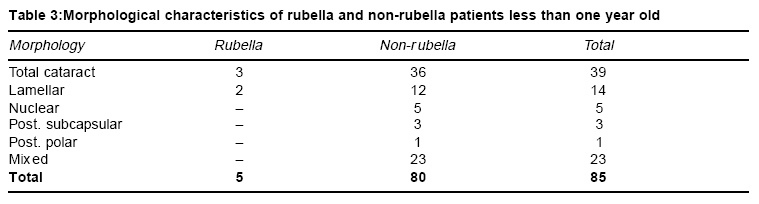
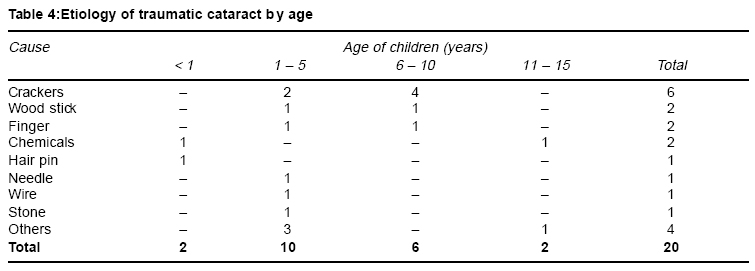
Accepted Date: 25-03-2004 Code Number: ms04018 Abstract Background: Cataract is responsible for about 10% blindness among children in India. Etiology of cataract is not well defined especially for childhood cataracts and epidemiological data for Indian population is not available in details. Aim: This study was performed to survey the causes of childhood cataracts and to identify the preventable factors in four western states of India. Settings and design: The present study is a hospital-based, prospective study on 172 consecutive pediatric cataract patients. Material and Methods: Type of cataract was determined using slit-lamp bio-microscopy or operation microscope after mild general anesthesia especially on very young babies. Other anomalies of eye were determined using appropriate ophthalmic instruments. Parents of the patients were interviewed in their native language using a standardized questionnaire. Biochemical and microbiological tests such as for rubella, reducing sugar and blood glucose were also performed. Results: Out of 172 children, 88.4% had non-traumatic cataract and 11.6% had traumatic cataracts. Among non-traumatic cataracts, 7.2% were hereditary, 4.6% were due to congenital rubella syndrome, 15.1% were secondary and 73.0% were undetermined. In the group of undetermined cases, during pregnancy 67% of the mother had history of illness, and 22% had taken medications during pregnancy. Conclusions: Our study shows that nearly 12% of non-traumatic cataract is due to potentially preventable causes. Health education of women to childbearing age and school children can decrease incidence of pediatric cataracts. Key Words: Etiology, Childhood cataract, Congenital cataract, Hereditary cataract, Rubella. INTRODUCTION Cataract is the opacification of the eye lens and based upon the age at appearance, cataract can be classified as congenital, infantile, juvenile, presenile and senile. Pediatric cataracts are responsible for more than 1 million childhood blindness in Asia.1 In developing countries like India, 7.4 - 15.3% of childhood blindness is due to cataract.2-4 The prevalence of cataract in children has been estimated between 1-15/10,000 children.5 Hereditary, metabolic and other ocular or systemic disorders and trauma are known factors responsible for cataract in children.6 In India, half of all childhood cataracts are Idiopathic.7 Inadequate awareness of the causative factors of cataracts within the society has lead to proliferation of cataracts in children. Childhood cataracts may have genetic or non-genetic bases. They may be inherited either as a non-syndromic ocular abnormality or may be associated with numbers of other ocular or multisystem disorders. Relatively little information on childhood cataract is available from developing countries. Few studies have been carried out to know the etiology of congenital cataracts in India.2-4, 9,10,12 However there is no report on the etiology of childhood cataracts in western India. In light of complexity in the etiology of pediatric cataracts, the present hospital-based study was performed to identify the causes of childhood cataract in patients from four different states of western India with an emphasis on factors that may be preventable, of proper education and training are given to parents and young children. MATERIAL AND METHODS This prospective observational study comprises of 172 patients with cataracts, aged between 10 days to 15 years. The patients with congenital unilateral and bilateral cataracts and traumatic cataracts residing in any of the four western states of India (Gujarat, Rajasthan, Madhya Pradesh and Maharastra) who have visited centre from February 2001 to March 2002 were included in the present study. A team of ophthalmologists and pediatricians attached to the centre examined all the patients preoperatively. For preoperative examination, the pupil was dilated using atropine eye drops. Children who did not cooperate were examined by giving them short-term general anesthesia under operating microscope. The type of cataract was determined using slit lamp bio-microscopy or operating microscope. To find out any other ocular pathology, vertical-horizontal corneal diameter, intraocular pressure, keratometry, axial length were measured and fundus status evaluated with indirect ophthalmoscope. Biochemical investigations such as urine sugar and blood glucose level were performed in all patients. Reducing sugar of urine sugar was measured by Benedict's test.8 Blood glucose level was measured by glucose oxidase peroxidase method using commercially available kit (Autospan, Span Diagnostics Ltd, Surat, India). TORCH test was done only in children less than one year of age with central nuclear or total cataract unilaterally or bilaterally and whose mothers revealed a history of illness accompanied by a rash during the pregnancy. The TORCH test was done using IgG and IgM antibodies by ELISA method, using commercially available kits (Radim S. A., Parc Scientifique du Sart Tilman, Angleur, Belgium). Some patients were diagnosed positive for rubella prior to their visit to the centre. The complete clinical details of the patient including cataract type and other ocular and non-ocular disorders and laboratory investigations were recorded in the proband's case sheet. A single trained interviewer using standardized questionnaire interviewed parents of all patients in the local language. Information regarding proband's cataract history, parental health history, prenatal and postnatal history, child's birth history, consanguinity, socio-economic and demographic status were also noted in the questionnaire. Completed questionnaire and proband's case sheet were filed together. In case of positive family history, affected siblings, parents and near relatives were also examined and noted in proband's case sheet. Suggestions of institutional ethical committee were strictly followed and informed consent was obtained from all the families included in this study. Clinical information of all patients was analyzed according to their etiology. The cases were divided into traumatic and non-traumatic. The traumatic patients were further classified based on the causes of trauma. The non-traumatic cases were classified into four groups based on the following considerations. A. Hereditary: This group included cases with positive family history. B. Secondary: This group-included case with any other ocular disease, metabolic systemic diseases, and cataracts associated with known syndromes. The syndromic cataracts were determined based on the clinical observation. The metabolic disorders were confirmed by the proband's history and earlier diagnosis of referring pediatrician. C. Rubella: This group-included cases caused by diagnostically confirmed congenital rubella syndrome. D. Undetermined: This group included idiopathic cases with no known cause. RESULTS In the present etiological study, out of 172 children with cataract, 88.4% cataracts were on-traumatic and 11.6% were caused by trauma. 54.65% were below one year of age while remaining 45.35% were more than one year of age. Male patients were two times more than female patients (117 boys: 55 girls). Non-traumatic cataract The ratio between bilateral and unilateral cataracts in children with non-traumatic cataract was 116: 36 (3:1). Out of 116 children with bilateral cataract at least 65 (58%) were congenital. The causes of non-traumatic cataract are shown in Table 1. The definite cause of cataract could not be determined in 73% cases even after detailed examination and investigations. 7.2% had hereditary cataract and 4.6% had congenital rubella syndrome. Secondary cataracts were found in 15.1% cases. Morphological types of non-traumatic cataracts in 152 children were blue dot 2 (1.31%), lamellar 32 (21.05%), mixed 40 (26.31%), nuclear 13 (8.55%), post-polar 3 (1.97%), post-subcapular 7 (4.60%), sutural 1 (0.65%) and total 54 (35.52%). Hereditary cataract: 11 (7.2%) cases had a family history of cataracts. On the basis of pedigree of the family, autosomal dominant cataract was confirmed. Information on the age at onset of cataract of all affected family members revealed the nature of cataract as congenital. 46% of the patients had total, 18% lamellar, blue-dot and nuclear in 9% each and remaining 18% had mixed type of cataract. In three cases of twins the morphological characteristics of the cataract were identical. Parents of seven children were consanguineous but none of the cases revealed history of inherited cataract. Secondary cataract Cataract secondary to uveitis, persistent hyperplastic primary vitreous, aniridia and others was found in 7 (4.6%) cases of non-traumatic cataract. The Down, Marfan and Lowe syndromes were associated with cataract in 3 (2%) children. There were 12 (7.9%) children who had central nervous system (CNS) abnormalities manifesting as grossly delayed milestones or epilepsy. One case had galactosemic cataract that was confirmed by laboratory tests. Rubella cataract Table 2 represents the cause of cataract in children less than 1 year of age. We carried out TORCH test for rubella in 63 patients out of 152 patients of non-traumatic cataracts and out of them 7 were found positive for the rubella. 5 children were less than one year of age at the time of presentation while 2 cases presented to us at the age of 7 and 8.5 years respectively. The morphological characteristics of cataracts in children under 1 year old with and without rubella are presented in Table 3. In confirmed congenital rubella syndrome cases, the observed morphology of cataract was total (3) and lamellar (2). Eight mothers revealed a positive history of skin rash during pregnancy, out of which one child was positive for rubella antigen. Undetermined causes: In the group of children with cataract of undetermined category, systemic illness of the mother during pregnancy may be important. 15.8% of mother of children with idiopathic cataract had toxemia of pregnancy, 22% had fever with rigors during the gestation period, of which 12 patients suffered during 2 to 6 month while 16 during 6 to 9 months of gestation. 9.4% had pulmonary tuberculosis and 8.7% had arthritis. 9.4% had skin rash during pregnancy. Skin rash was present in 9.4% mothers during first and second trimester of pregnancy. The percentage of the mothers who had taken medicine during pregnancy and abortifacients during first trimester is 22% and 3.2% respectively. Traumatic cataract Out of 20 children with traumatic cataract 16 (80%) were boys. 75% of the children with traumatic cataract were from urban areas. The types of injuries and age of the children at the time of trauma are shown in Table 4. 60% of the traumatic cataract occurred in children below 5 years. Penetrating injuries contributed 40% of traumatic cataract cases while blunt injuries were found in 60% cases. Play related injuries (80%) were most common compare to that of work related injuries (20%). DISCUSSION Many etiological studies on childhood cataract have been carried out in developed as well as developing countries to determined causative factors.7,9 -12 Studies performed in various parts of India shows variation in etiological factors affecting childhood cataract. In south India among non-traumatic cataracts, 25% were due to hereditary, 15% were due to congenital rubella syndrome and 51% were idiopathic. Nearly half of non-traumatic cataracts in this population are due to potentially preventable causes like congenital rubella syndrome and autosomal dominant disease.9 In North India, Angra (1987) found that 31% were idiopathic, 14% were hereditary and 21% may have been due to rubella.12 While Jain et al. (1983) found that 20% were hereditary, 9% were due to metabolic diseases and 5% had cataract associated with known syndrome.10 We found that among non-traumatic cataracts, 7.2% were due to hereditary, 4.6% were due to congenital rubella syndrome, 14.5% were secondary cataract and more than 50% cases were idiopathic. The percentage of hereditary cataracts is lowest in our study. According to previous study reported that other ocular abnormalities are associated with genetic cataract.6 9% of the eyes with inherited cataract had an association with microphthalmos9 while no such association was found in our study. Such observations revealed that the genetic abnormalities in the different regions of the Indian population may be different. The occurrence of hereditary cataract, congenital rubella syndrome, galactosemia is less compare to the previous studies in north India and south India.9,12 The occurrence of cataracts in the consanguineous marriages is less in the present study compared to previous reported studies.13,14 It may be due to the fact that such type of marriages are not common in this part of India. Rubella is a common cause of cataract blindness in south India and accounts for more than 25% of all new cases of congenital cataract.9 In our study we found that 4.6% cases of congenital cataract is due to rubella which is much more less than 15% and 21% reported in south9 and north Inida12 respectively. It appears that prevalence of rubella may be less in patients from western India compare to those from north and south India. Rubella cataracts show generally nuclear opacity9, but in the present study we also found total and lamellar opacity. Galactosaemia is the most common metabolic disturbance causes paediatric cataracts. In the present study only one case (0.6%) among non-traumatic cataracts was positive for urine reducing sugars however, Angra (1987) reported a higher frequency (2.5%) of sugar cataracts among congenital cataract from north India.12 Majority of childhood cataracts in western India are idiopathic. The ingestion of corticosteroids, antibiotics, anti-diabetic drugs, others (busulfan, triparanol, chlorpromazine, dinitrophenol, etc.) has been implicated as a cataractogenic factor by a number of studies. Use of abortifacients is also cited as a cause of congenital cataract.12 In case of premature infants, transient congenital cataract occurs occasionally and such condition may be associated with low birth weight, birth anoxia or CNS involvement.15 In order to know possible association between medications during pregnancy and cataract, we collected information regarding maternal illness and drug ingestion during pregnancy. However, we couldn't establish significant correlation due to lack of accurate history of drug ingestion and details of composition of drug. Drug was taken during pregnancy in 22% cases however, precise information about drugs was not known. Among undetermined cases we found that 21 (16%) cases were born prematurely. Seven cases were associated with low birth weight and 2 had CNS abnormalities. Finally we conclude that around 12% of non-traumatic bilateral cataracts in western India are due to potentially preventable causes. Further studies are required to identify factors leading to childhood cataract in more than fifty percent of the cases for which definite cataractogenic factor could not be determined. Awareness programs for pregnant women for concerning precautions during pregnancy and also for keeping records of medications taken during pregnancy might help in future etiological studies. School children must also be educated for factors, which can cause traumatic cataract, which might reduce the incidences of childhood cataract. REFERENCES
Copyright by The Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04018t4.jpg] [ms04018t2.jpg] [ms04018t3.jpg] [ms04018t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}