 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Science Vol. 58 No. 5, May, 2004, pp. 196-202 MINI LAPAROTOMY VERSUS CONVENTIONAL LAPAROTOMY FOR ABDOMINAL HYSTERECTOMY: A COMPARATIVE STUDY JAI BHAGWAN SHARMA, LEENA WADHWA, MONIKA MALHOTRA, RAKSHA ARORA Deptment of Obstetrics and Gynecology. Maulana Azad Medical College
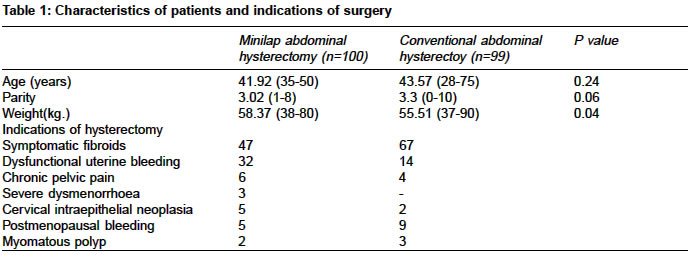
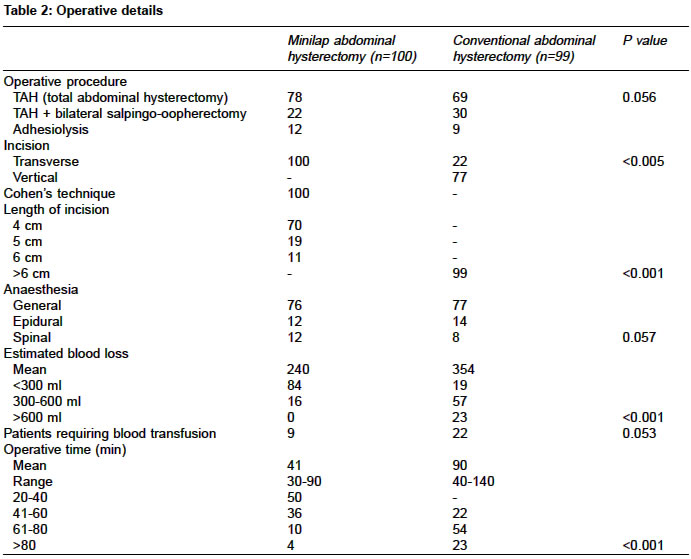
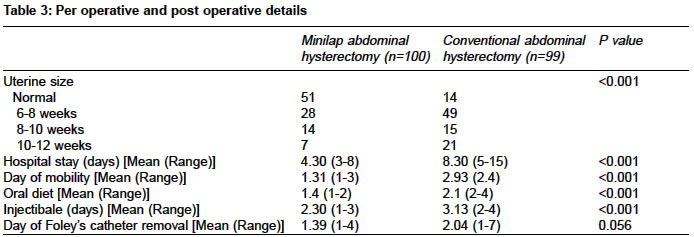
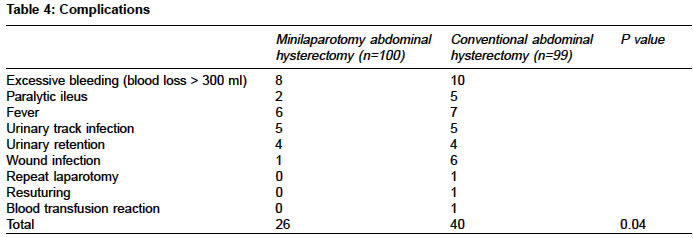
Associated Lok Nayak Hospital, New Delhi - 110002, India Code Number: ms04035 ABSTRACT Background: Less traumatizing measures for hysterectomies are searched for to improve the recovery from surgery. Aim: Comparison of minilaparotomy abdominal hysterectomy with conventional abdominal hysterectomy in respect to per-operative and post-operative outcome and complications. Setting and Design: In a medical college hospital patients undergoing abdominal hysterectomy were enrolled. It was a concomitant comparative study. Methods and Material: We are presenting our comparative data of 100 cases of minilaparotomy abdominal hysterectomy (group I, incision =< 6 cm) performed over last 4 years from January 1998 to December 2002 and comparing the outcome with 99 cases of abdominal hysterectomy (group II, incision > 6 cm) done by traditional method over the same duration. Statistical analysis used: Chi-square and Fischer test with significance of p value being taken at 0.05 were used for categorical data, while student's t test was used for continuous data. Results: Mean age and parity of patients were similar in the two groups. Incision was transverse in 100% cases in-group I and 22.2% cases in-group II. Estimated blood loss was significantly higher (354 ml) in group II in contrast to group I (240 ml). Blood transfusion was also required more commonly (22.2%) in-group II than in-group I (9%). Mean operative time was significantly more in-group II (90 minutes) than in group I (41 minutes). Mean hospital stay, day of mobility, starting oral diet and days of injectable analgesics required were higher in group II than in group I. Major complications were rare in both the groups, but minor complications were significantly higher in group II (40.4%) than in group I (26%). Conclusion: Minilaparotomy abdominal hysterectomy appears to be an attractive alternative to traditional abdominal hysterectomy with fewer complications. Key Words: Hysterectomy, Minilaparotomy, Laparotomy, complications. INTRODUCTION Hysterectomy is a common gynecological operation with almost 20% of British women having undergone it by the age of 65 years 1 Till recently, the choice of hysterectomy was limited, abdominal hysterectomy was performed for all benign and malignant gynecological disorders, while vaginal hysterectomy was done for prolapse cases.1-5 Lately, vaginal hysterectomy has been widely used for otherwise uncomplicated hysterectomies. Laparoscopic assisted vaginal hysterectomy (LAVH) and laparoscopic hysterectomy have recently become popular due to shorter hospital stay and minimum post-operative morbidity but needs extensive training and expensive equipments.2,3,6 Minilaparotomy has been used for sterilization operations for decades and is an established technique7. Minilaparotomy has been used for many benign gynecological conditions, reversal of sterilization and ovarian cysts with encouraging results8-10. However, there is very scant literature available on minilaparotomy hysterectomy in the world literature11. There is a need to know whether minilaparotomy hysterectomy is safe and cost effective in contrast to standard abdominal hysterectomy. In the present study, Primary outcomes measured were - Mean operative time and blood loss. Secondary outcomes measured were: - Days of hospital stay, day of mobility, day of starting oral diet, days of injectable analgesic, days of removal of Foleys catheter and overall complications rate in both groups. The purpose of this study was to determine the feasibility and acceptability of minilaparotomy abdominal hysterectomy for selected patients. This is the first report to our knowledge, which compares the results of minilaparotomy hysterectomy with conventional abdominal hysterectomy. MATERIAL AND METHODS This was a prospective non-randomized comparative study between minilaparotomy hysterectomy (group-1) and traditional abdominal hysterectomy (group-II) for upto 12 weeks sized uterus over last 4 years from January 1998 to December 2002 in gynecology department. Taking into consideration other studies on various modes of hysterectomy from the world literature and the various complication rates, power analysis was performed to avoid bias from chance factors and a sample of 75 patients in each group was calculated. Thus, it was proposed to enroll 100 and 99 patients in each arm. The Inclusion criterion was small mobile uterus (upto 12 weeks size). Exclusion criteria were patients with previous surgery, with malignancy and large adnexal masses, patients with genital tuberculosis and those not willing for study were excluded. Written informed consent was taken from all the patients and the departmental ethical committee approved the study. All the operations were performed by either a consultant or by at least a Senior Resident with consultant assisting and supervising and by one of the authors of the study. Minilaparotomy hysterectomy (incision =< 6 cm) was performed using uterine holding clamps with uterus delivered outside the abdominal wall. Conventional abdominal hysterectomy was performed in traditional manner4. Intraoperative blood loss was estimated by measuring blood in the suction bottles and by the number of packs soaked during the surgery. Patients were encouraged to ambulate as early as possible but when they felt themselves ready for ambulation. All patients were given general anaesthesia for the surgery and were given post operative pain relief on demand but not more than three doses of injection Diclofenac in 24 hours. Patients were encouraged to start oral fluids from next morning when bowel sounds appeared and semi-solid diet from second day after noon. Blood transfusion was given during surgery if blood loss was more than 500 ml. The patients were allowed to go home if they had no complications, were ambulatory, were eating well and had moved their bowels. Preoperative and postoperative outcome and complications were compared in the two groups. Statistical analysis: The data were tabulated and analyzed. Summary statistics such as mean, standard deviation were estimated. Chi-square test and Fisher's exact tests were used for categorical data. For continuous data like age, weight, blood loss, duration of surgery, student's t test was used. As the sample size was large enough so Mann Whitney test was not applied. The significance was seen after applying log transformation. RESULTS The characteristics of the women and indications of the hysterectomy are given in table 1. There was no significant difference in the mean age and parity of women in the two groups. Weight was significantly higher in group I than in group II. Main indications were symptomatic fibroids or dysfunctional uterine bleeding. The operative details are given in table 2. The surgery performed was total hysterectomy, with or without bilateral salpingo-oopherectomy and with or without adhesiolysis. Incision given was transverse less than 6 cms (definition of minilaparotomy) in all 100 cases in-group I, while it was vertical in 77 women in-group II. There was no difference in the type of anaesthesia in the two groups. The estimated blood loss was significantly higher (354 ml) in group II in contrast to group I (240 ml) and need of blood transfusion was significantly higher in group II (22.2%) than in group I (9%). Mean operating time was significantly higher (90 minutes) in-group II than in group I (41 minutes). The preoperative and postoperative details are given in table 3. Uterine size was significantly bigger in group II than in group I. The mean hospital stay, day of mobility, day of starting oral diet and days of injectable analgesic was significantly higher in group II than in group I. There was no significant difference in the days of removal of Foley's catheter and type of antibiotics used in the two groups. The postoperative complications are shown in table 4. Major complications were rare in both the groups. Overall complications rate was significantly higher (40.4%) in traditional abdominal hysterectomy than in minilaparotomy hysterectomy (26%). DISCUSSION In the present study, mean operating time, mean hospital stay, day of mobility, day of starting oral diet and maximum injectable analgesics required were higher in conventional laparotomy than in minilaparotomy group. Hysterectomy is a common operation, which can be done by abdominal or vaginal route. There have been few studies only comparing vaginal and abdominal hysterectomy. The famous CREST study conducted by the Center for Disease Control in 1982 showed overall complication rate for women undergoing vaginal hysterectomy to be 24.5 per 100 women compared with 42.8 per 100 women undergoing abdominal hysterectomy and the risk of having one or more complication was 1.7 times more likely in the abdominal hysterectomy group.4 Till date no study has compared minilaparotomy abdominal hysterectomy with abdominal hysterectomy. The present study was only a comparative study of two techniques done on different patients concomitantly but not a randomized controlled study, which was a limiting factor of the present study. The mean operative time and blood loss was lower in minilaparotomy than in traditional abdominal hysterectomy. The recovery was quicker with less hospitalization and fewer complications in the minilaparotomy group. Complication rate was lower in the minilaparotomy group as was the time taken for surgery and blood loss. The febrile morbidity in our study was much lower than in Dicker et al.4 This may be because of routine use of antibiotics to all patients in our study and that the study by Dicker et al was done in 1982. Garry et al5 (2004) compared laparoscopic hysterectomy with abdominal and vaginal hysterectomy and concluded that laparoscopic hysterectomy was associated with a significantly higher rate of major complications than abdominal hysterectomy. It also took longer to perform but was associated with less pain, quicker recovery and better short-term quality of life. The trial comparing vaginal hysterectomy with laparoscopic hysterectomy was inconclusive. However, vaginal hysterectomy took less time. Purohit6 Technique of Vaginal Hysterectomy for benign disease of the uterus without prolapse (excluding endometriosis and uteri above 20 week size) was found to be easy, safe and effective. Vaginal hysterectomy is associated with decreased trauma as expressed by lower trauma markers compared to abdominal hysterectomy.10 Postoperative complications were fever in 2 patients, ileus and atrial fibrillation in one patient each in Hoffman and Lynch study 11 while these were fever (6 cases), paralytic ileus (2 cases), urinary tract infections (5 cases), urinary retention (4 cases), wound infection (1 case) respectively in the present study. Mean day of ambulation, start of oral diet and discharge were 1.3 days, 2.4 days and 3.4 days respectively in Hoffman and Lynch study in contrast to 1.3 days, 1.4 days and 4.3 days respectively in the present study in cases of minilaparotomy hysterectomy. The present study was not a randomized controlled study but was only a comparative prospective study. There were patients with vertical incision in-group II which might have biased the result as vertical incision may be associated with increased post-operative morbidity in contrast to transverse incision. Similarly, the size of the uterus operated was larger in-group II than in-group I which might have been responsible for increased post-operative morbidity in-group II. Hence it's concluded from the present study that minilaparotomy hysterectomy was associated with minimum per-operative and postoperative complications while abdominal hysterectomy had more problems. Although minilapartomy has been used for tubal sterilization for some time, its application to benign gynecological disorder is recent. It can be used for selected group of patients as mentioned in inclusion criteria. This procedure would seem to have great potential for use in third world countries as it can been learnt easily and can be done. Although the present study suggests better patient outcome with minilaparotomy hysterectomy than with conventional abdominal hysterectomy, it was a non-randomized study. Prospective randomized controlled studies are recommended for future research. REFERENCES
Copyright by The Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04035t4.jpg] [ms04035t2.jpg] [ms04035t3.jpg] [ms04035t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}