 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Science Vol. 58 No. 5, May, 2004, pp. 206-210 CASE REPORT MALIGNANT STRUMA OVARII: A CASE REPORT AND REVIEW OF THE LITERATURE MA OSMANAGAOGLU, H BOZKAYA, A REIS Departments of Obstetrics and Gynecology and Pathology, Karadeniz
Technical University, Faculty of Medicine, Trabzon, Turkey.
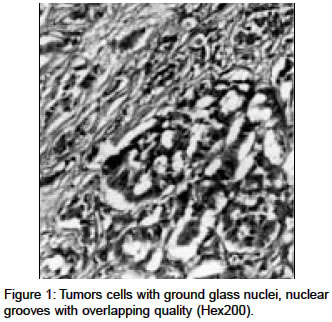
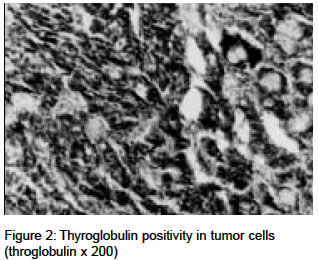
Code Number: ms04037 ABSTRACT A 45-year-old woman with papillary carcinoma arising in struma ovarii which involved one ovary without dissemination is presented. Total abdominal hysterectomy and bilateral salpingo-oophorectomy were performed. Histopathological examination revealed malignant struma ovarii of the papillary type. The flow cytometric analysis revealed an hypodiploid DNA content (DNA index:0.67). Since these are rare tumors, there is no universal exact protocol for the treatment and follow-up of patients with malignant struma ovarii. More data are needed to determine the prognosis and management in preferring mode of therapy. Key Words: Malignant struma ovarii, papillary carcinoma, aneuploidy INTRODUCTION Struma ovarii is a highly specialized form of mature ovarian teratoma. While approximately 15% of teratomas contain thyroid tissue, struma ovarii can only be diagnosed when thyroid tissue is the predominant element.1,2,3 Malignant struma ovarii is very rare; only a few cases with clinically evident metastatic disease are documented in the literature.1,2,3 We report a case with papillary struma ovarii observed in an ovary teratoma without metastatic dissemination. CASE REPORT A 45-year-old woman, gravida 2, para 2 was admitted to our clinic for abnormal uterine bleeding (menometrorrhagia and postcoital bleeding). Her medical and family histories were unremarkable. At the time of admission, her physical and genital examinations showed no abnormalities. On pelvic examination a normal vagina, a cervical polyp of the isthmus of the cervical canal about 0.5x0.5 cm in size and unremarkable uterus were observed. A mass extending from the right adnexa could be palpated. Prior to surgery the patient did not show any symptoms of thyroid hyperfunction. Transvaginal ultrasound examination revealed a somewhat enlarged uterus with 12-mm-thick endometrium and there was in the right ovary a 63 x 46 mm cystic mass. Her laboratory results were unremarkable. The patient had normal pap smear. A dilatation and curettage was performed for the polyp and showed normal endometrium with cervical polyp. The plasma level of CA-125 was 18 IU/ml (reference value <35 IU/mL). The patient underwent a total abdominal hysterectomy and bilateral salpingo-oophorectomy (TAH/BSO) for her adnexal mass. Intraoperatively, the uterus, left ovary and bilaterally tubes were normal. There was a irregular cystic mass of right ovary measuring 60x70 mm. There was no palpated lynph nodes during surgery. Frozen section diagnosis of the omental, peritoneal biopsies and right salpingo-oopherectomy material was reported to be mature teratoma with benign thyroid tissue. The peritoneal washing was negative by cytological examination. Postoperative course was uneventfull. On macroscopic examination, a tumor of the right ovary, 5 x 6 x 6 cm was found and the cut surface demonstrated cystic spaces and colloid rich solid areas. Uterus, left ovary and bilateral tubes were within normal limits. Histopathological examination of postoperative specimen revealed tumor tissue with mature squamous epithelium skin adnexae and thyroid tissue composed of follicles. The epithelium of follicules show papillary and follicular patern with typical nuclear characteristics including ground glass (optically clear) nuclei with overlapping quality and nuclea grooves (Figure 1). The left ovary and the uterus were unremarkable. Tumor cells were immunoreactive with thyroglobulin (Figure 2). Detailed examination of the throid gland was performed. Thyroid function tests, thyroglobulin level and findings of ultrasonography were in the normal range. Flow cytometric DNA analysis was performed on tissue removed from paraffin-embedded tissue blocks and determined aneuploid DNA content (DNA index:0.67, hypodiploidy). On follow-up, the patient did not reveal any abnormalities in 48 months. Antibodies of antimicrosomal and antityroglobulin levels were in the normal range. The thyroid function tests (six monthly with physical examination and thyroid ultrasonography) and serum thyroglobulin levels (at six months interval<56ng/ml), performed subsequent to surgery were within normal limits. At 6 month intervals repeated of computed tomography (CT) scan of the abdomen and chest were unremarquable. A 2.5mCi diagnostic 131I whole body scannig (WBS) with thyroid stimulating hormone (TSH) stimulation 12 months after surgery and repeated annually showed no up take in the abdomen, chest or in the neck outside the thyroid gland. DISCUSSION There are no uniform diagnostic criteria for malignant struma ovarii, Devaney et al4 however, insisted that diagnosis should be reserved for lesions that exhibit the full range of changes seen in thyroid carcinoma emphasized the presence of cytologically overlapping `ground glass' nuclei and mitotic activity or vascular invasion thus reducing the incidence of disease and unwarranted treatment. Immunohistochemical stains for thyroglobulin is important to use because solid and microfollicular areas of the struma ovarii must be differentiated from carcinoid and granulosa cell tumors (Figure 2). But, the presence of throglobulin in tumor does not result in the differentiation of struma ovarii as malignant or benign.1 Preoperatively, the clinical diagnosis of struma ovarii is possible in patients having hyperthyroidism, but only 8 % of patient with struma ovarii present with clinical hyperthyroidism.2 Although CA-125 level was seen generally in normal range, in some patients with struma ovarii, its level was elevated which may lead to suspicion of an ovarian malignancy.5 It is difficult to distinguish between struma ovarii and dermoid cysts on the basis of their sonographic appearance. Struma ovarii has some characteristic magnetic resonance appearance of a multilobulated complex mass with thickened septa, multiple cysts of variable signal intensities, and enhancing solid components.6 In the present case, preoperatively, there was no suspicous of malignancy. Thyroglobulin level and TSH-stimulated low-dose 131I whole-body scanning have been found to be a valuable sensitive and indicative of persistent and recurrent thyroid carcinoma7. In most patients, both methods give concordant results, however, in some patients, thyroglobulin is measurable, but the diagnostic scan with 131I is normal3 and both methods have limitations when the patients had a thyroid remnant, when serum thyrotropin was not suppressed, and in cases of local recurrence. It is also important to make sure that the thyroglobulin is not falsely elevated as a result of antibodies. In this case, the solid component with histologically malignant features revealed an aneuploid DNA content (DNA index:1.6, hyperdiploidy), while benign component was diploid8. However, there is no adequate data on DNA aneuploidy which is significant to determination the prognosis of malignant struma ovarii. Because of the rarity of the malignant struma ovarii the optimal surgical and postoperative management has not been well defined. Therapy ranged from radical surgery and radio-chemotherapy, laparoscopic staging with surgery, to conservative surgery in younger patients with a desire to preserve fertility if disease is confined to the ovary and after completion of childbearing, treatment followed by TAH/BSO, lymph node dissection and omentectomy.3,9 Additionally, DeSimone et al7 have proposed radical surgery including thyroidectomy to enable effective 131I ablative treatment and to facilitate follow-up with serial 131I diagnostic WBSs and serum throglobulin measurements with also exclusion of a primary thyroid carcinoma followed by 131I therapy in advanced disease. We believe that conservative surgery for women of childbearing age is an option. After completion of childbearing and for all others, we recommend TAH/BSO, sampling of pelvic and para-aortic lymph nodes, peritoneal cytologic washing and partial or total omentectomy. In patients who have stage IA malignant struma ovarii with no evidence for residual disease on physical examination, on the first 131I WBS scan or thyroglobulin testing, follow-up may be scheduled at yearly intervals with the traditional diagnostic methodologies. If recurrence or more advanced disease have been demonstrated, according to the current management of thyroid carcinoma, thyroidectomy and ablation with 131I therapy and suppressive thyroid hormon therapy thereafter is recommended. Since these are rare tumors, there is no universal exact protocol for the treatment and follow-up of patients with malignant struma ovarii, therefore more data are needed to determine the prognosis and management. REFERENCES
Copyright by The Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04037f2.jpg] [ms04037f1.jpg] |
| |||||||||

{kind=link}
{kind=link}