 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Science Vol. 58 No. 5, May, 2004, pp. 214-216 Practitioners Section Iron deficiency anemia - Part III Asha Shah MD (Med), DNB (Med), Consultant Hematologist, BSES MG Hospital
and Holy Family Hospital, Mumbai, India.
Accepted Date: 28-04-2004 Code Number: ms04040 Treatment Treatment of iron deficiency anemia should include
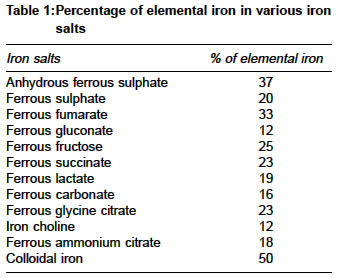
1. Treatment of the cause It is important to find out the etiological factor of iron deficiency to prevent failure of treatment and recurrence of iron deficiency after stopping treatment. Treatment of worms especially ankylostomiasis or hook worm infection, giardiasis, bleeding from any sites, recurrent infections, is very essential to prevent recurrence. In case of hook worm infection, watch should be also kept for re infection which should be treated periodically. Bleeding from `piles' is another common cause of iron deficiency anemia (IDA) among adults which should be treated by injection or excision. All pregnant women should be started on iron supplements very early in pregnancy and should be continued throughout pregnancy, postpartum period and till she continues to breastfeed her baby. Patient should be advised to prevent repeated pregnancies at short intervals. Patient should be advised against abuse of `pain killers' especially aspirin as it is a common cause of GI bleed and iron deficiency. 2. Correction of anemia Iron deficiency can be easily corrected in a majority of patients with iron therapy. This treatment can be given either by oral or parenteral route. Oral iron therapy Iron is usually given in dose of about 200 mg of elemental iron per day in single or divided doses. It is preferably given on empty stomach or between meals to facilitate absorption, but if the patient complains of GI side effects it is better to administer it after meals, although this approach would also reduce the absorption of iron. Doses higher than 200 mg per day are not recommended as it would not be more effective but only give rise to more side effects. Once the patient is started on oral iron therapy, it takes about 6 10 weeks for hemoglobin to return to normal level. However in IDA, iron stores are exhausted and need to be replenished. Replenishment of iron stores begins only after hemoglobin returns to normal. Hence stopping iron soon after hemoglobin is normal means inadequate therapy and predisposes patient to recurrence. Absorption of iron diminishes after hemoglobin returns to normal and hence replenishing iron stores is a very slow process and takes about 3 - 4 months. Thus iron therapy should be continued for 5 - 6 months. Iron preparations Various types of iron salts are available as shown in Table 1. Of these ferrous salts are preferred as they are better absorbed than ferric forms. There is no significant difference in absorption when a ferrous salt of iron is given in the form of sulphate, gluconate, lactate, fumarate or succinate, but iron is poorly absorbed in the form of carbonate, citrate and pyrophosphate, in ferric forms, colloidal iron preparations and as iron carbohydrate complexes. Various forms of preparations are available including tablets, capsules, drops, syrups, sugar coated tablets, slow release tablets and chewable tablets. Uncoated tablets and sugar coated tablets eg. fersolate are least expensive and well absorbed. Liquid preparations are in the form of syrups and drops. These are expensive and deteriorate on storage, but are useful for administration to infants and children who cannot swallow tablets. They usually lead to temporary staining of teeth and tongue which disappears on discontinuation of the drug. Iron in slow release form is supposed to reduce the side effects of iron therapy. Side effects of oral iron therapy are few and experienced by a very small minority. Absorption of iron is maximum from the duodenum and hence absorption of iron from prolonged release preparations is reduced as iron is released lower down in the gut. The cost of these sustained-action preparations is comparatively high. Slow release preparations , thus, are more expensive and less effective. Combination of iron with other nutrients like ascorbic acid, vitamins and folic acid increases the cost as well as increases the frequency of side effects and hence non-compliance. Hence it is best to give iron alone as ferrous salt very effective and least expensive. Side Effects of oral iron Major side effects of oral administration include epigastric pain, nausea, vomiting, abdominal cramps, diarrhea, and constipation. By and large the side effects are less, and it is well tolerated if proper counseling is done before starting the therapy. In many cases side effects are psychological in origin. It was shown in a trial that these patients develop side effects even when given placebo therapy. Many patients, who do not tolerate iron, do not get any side effects if they are unaware that they are taking iron. Thus many side effects are exaggerated mainly by those who claim their compound has lesser side effects. Side effects of oral iron are directly related to the amount of elemental iron, administered. Hence side effects are much less with ferrous gluconate, iron choline citrate and ferrous calcium citrate which have much lower elemental iron content than anhydrous ferrous sulphate (Table 1). Of late people have tried twice a week therapy which has proved to be equally effective with fewer side effects. Parenteral Iron Therapy Indications There are very few indications for parenteral iron therapy. It is indicated when the patient does not tolerate oral iron which is uncommon. It is indicated when a pregnant woman presents with severe anemia in the last month of pregnancy which again would be rare if proper antenatal care is taken at earlier stages of pregnancy. Another indication for iron injection is intermittent massive or continuous slow blood loss through the gastro-intestinal tract due to inoperable conditions e.g. intestinal polyposis or hereditary hemorrhagic telangiectasis. Such patients may receive several grams of iron over period of years to keep up their hemoglobin. Lack of response to oral therapy is not an adequate indication for parenteral therapy unless it is shown that this is due to malabsorption of iron which is rare. Parenteral therapy includes both intramuscular and intravenous iron therapy Intramuscular preparations Jectofer and Imferon can be given intramuscularly. These are given deep into the upper outer quadrant of the buttock and the skin should be laterally displaced before injection (Z track technique) to prevent staining of the skin. Intravenous preparations Imferon can also be given intravenously in the form of a drip. In this manner, total requirement of iron can be given in single sitting. It is essential to give a small test dose intravenously before giving the total dose. Adrenaline should be kept ready in a syringe to counter anaphylactoid reactions while giving intravenous imferon. Calculation of the total dose of iron The simplest formula to calculate total dose of iron is: total dose of elemental iron (mg) = weight in kg X hemoglobin deficit X 4. It is customary to add 1000 mg to above to replenish iron stores. Side Effects of parenteral iron Fever, arthralgias, nausea, vomiting, diarrhea, body ache, skin rash, chest pain, abdominal pain, lymphadenopathy, angioneurotic edema, anaphylactic shock which has even lead to death in few cases. Intramuscular deposition of iron dextran has led to malignancy in experimental animals. Sarcomas have developed in humans also on rare occasions, at the site of iron injection. Prevention of IDA Various approaches will have to be taken both at individual level in the form of dietary modifications and iron supplementation, and at community level in the form mass education to spread awareness and ultimately, food fortification. Copyright by The Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04040t1.jpg] |
| |||||||||

{kind=link}