 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
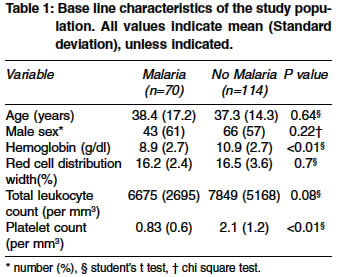
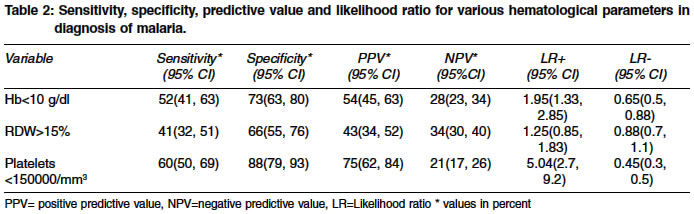
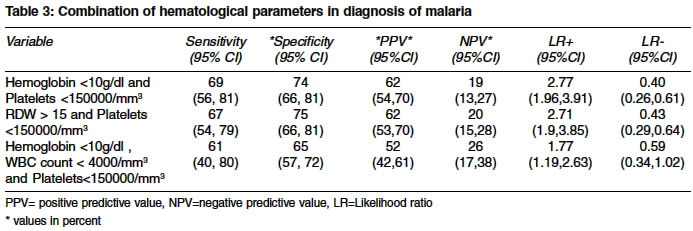
Indian Journal of Medical Sciences, Vol. 58, No. 6, June, 2004, pp. 239-244 Original Article Can hematological parameters discriminate malaria from nonmalarious acute febrile illness in the tropics? Lathia TB, Joshi R Department of Medicine, Mahatma Gandhi Institute of Medical Sciences, Sevagram, Maharashtra-442102 Code Number: ms04043 ABSTRACT BACKGROUND: Malaria is considered as the main differential diagnosis of acute febrile illness in the tropics, and alteration of various hem atological parameters has been observed in patients with malaria. AIM: To ascertain if certain hematological parameters increase the probability of malaria in patients with acute febrile illnesses. SETTINGS AND DESIGN: Hospital based, prospective cohort study. METHODS AND MATERIAL: All consecutive in patients with fever of less than seven days in duration were included in the study. Patients where localizing cause for fever could be determined were excluded. Hematological parameters (Hemoglobin, Red cell distribution width (RDW), Leukocyte count, and platelet counts) were determined by using automated counter, and peripheral smear examination for malarial parasite was taken as gold standard for the diagnosis of malaria. STATISTICAL ANALYSIS USED: Diagnostic accuracy was measured by computing sensitivity, specificity, predictive values and likelihood ratios. The precision of these estimates was evaluated using 95% confidence intervals. RESULTS AND CONCLUSIONS: A total of 184 patients were included in the study and 70 (38%) had a positive peripheral smear for malarial parasite. Thrombocytopenia alone (platelet countless than 150,000/mm3) was a predictor for malaria (Sn 60%, Sp 88%, LR+ 5.04) and in combination with anemia (Hb <10 g/dl) it was next best parameter (Sn 69%, Sp 74%, LR+ 2.77). RDW and leukocyte count were not predictive. The conclusion of this study is that the presence of thrombocytopenia in a patient with acute febrile illness increases the probability of malarial infection.BACKGROUND Malaria is a major health problem in the tropics with 300-500 million cases of malaria occurring annually, and an estimated 1.1-2.7 million deaths each year as a result of severe malaria.[1] In malaria patients a prompt and accurate diagnosis is the key to effective disease management. Clinical diagnosis, the most widely used approach for diagnosis of malaria in the tropics, is unreliable because the clinical presentation of malaria is diverse, and in a tropical country it may difficult to distinguish it from viral fever, arboviral infections, enteric fever or even leptospirosis.[2] Microscopic diagnosis, the established method for laboratory confirmation of malaria requires technical expertise and repeated smear examinations. It is a valuable technique when performed correctly but unreliable and wasteful when poorly executed.[2] The drug policy for malaria treatment under the National Anti Malaria Program in India is that any fever without any other obvious cause may be considered as malaria,investigated and treated accordingly, to prevent death and reduce malarial morbidity.[3] Especially in a chloroquine resistant era, early identification and treatment of malaria is imperative, hence the search for other diagnostic indicators. A variety of hematological alterations like progressively increasing anemia, thrombocytopenia,[4],[5] leukocytosis or leucopenia and rarely DIC have been reported in Plasmodium falciparum malaria.[6] The present study aims to detect if certain hematological indices would increase the probability of malaria in patients with acute febrile illness. Presence of such an indicator may heighten the suspicion for malaria, prompting a more diligent search for the malarial parasite, and prompt institution of specific therapy. Setting and Design METHOD AND MATERIALS All consenting consecutive patients who were admitted to the medicine wards with fever of acute onset (less than 7 days), between July and December 2003 were included in the study. Patient who had no fever recorded in the hospital stay, and those where a localizing cause (such as pneumonia, meningitis, skin or subcutaneous infections etc.) could be determined were excluded. All patients with fever were investigated with complete blood counts, serial peripheral smears on admission and at spike of fever, chest film, serum chemistry (electrolytes, creatinine and liver enzymes) blood culture and serology for salmonella. In addition cerebrospinal fluid examination, urine microscopy and culture, abdominal and brain imaging was done where indicated. The complete blood counts were done with an automated counter (Coulter), and peripheral smears were examined by a qualified pathologists. Pathologists were blinded to the automated coulter results. Four hematological parameters were taken as index tests (Hemoglobin, Red cell distribution width (RDW), total leukocyte count, and platelet count). Cut off value for low hemoglobin (Anemia) was taken as 10gm/dl,7 and high RDW was defined as a value more than 15%.[8] Total leukocyte count less than 4000/cu mm,9 and platelet count of less than 150,000/cu mm10 were used to define leucopenia, and thrombocytopenia respectively. Peripheral smear positive for malarial parasite was taken as a gold standard for the diagnosis of malaria. Statistical Analysis RESULTS A total of 184 patients of acute febrile illness without localizing signs were included in the study, 70 (38%) of them were positive for malarial parasite on peripheral smear examination and remaining114 patients were negative. Plasmodium falciparum was identified in 64 (34%) patients, and the rest had vivax malaria. Amongst patients with falciparum malaria, 21(32%) had cerebral malaria, three (4.6%) had acute renal failure, and other 40 (62%) had uncomplicated malaria. All six patients with vivax malaria had no complications. Of the 114 patients who were slide negative for malaria, 6 (5.2%) patients had enteric fever (positive blood cultures for salmonella typhi), 17 (14.9%) had probable enteric fever (Widal titers greater than 1:160), 36 (31%) patients were chloroquine responsive and another 23 (20.1%) had antibiotic responsive acute febrile illness. Presumptive diagnosis of viral encephalitis was kept in 32 (28%) patients (altered behavior, normal cerebrospinal fluid examination, and clinically non-responsive to antibiotics and anti-malarials). There was no difference in age, and sex profile in those who were slide positive for malaria vs those who were not [Table - 1]. Hemoglobin level and platelet counts were significantly lower in the patients with slide positive malaria in comparison to other fevers. We obtained sensitivity, specificity, predictive values, and likelihood ratio for diagnosis of malaria with hematological parameters as index test [Table - 2]. Presence of anemia, low leukocyte count, or high RDW had a poor sensitivity and specificity in diagnosis of malaria. Low platelet count (<150,000) was 60% sensitive and 88% specific for the diagnosis of malaria. This was the only discriminator parameter, with positive and negative likelihood ratio of 5.04, and 0.45 respectively. We used hematological parameters in combination to see if it increased the diagnostic yield. Combination of anemia and thrombocytopenia had higher sensitivity (69%), and a positive likelihood ratio of 2.77. The negative predictive value and LR- of this combination (19% and 0.40 respectively) argues that malaria may be ruled out if this combination is absent. Other combinations (High RDW &and low platelets, and low hemoglobin, low WBC count, & low platelets) also did not increase the diagnostic yield [Table - 3]. DISCUSSION The present study demonstrates that low hemoglobin and low platelet count are the two hematological variables that increase the probability of malaria, by factor of 1.95 and 5.04 respectively. These two variables also emerge useful when used in combination (Likelihood ratio 2.77). The 95% confidence interval for RDW however crosses one, which implies measurement of this parameter to be less precise. The low platelet count emerged as the strongest predictor of malaria, a previous observation which we confirm. In a study on over two thousand patients with fever, Erhart et al[11] reported platelet count of less than 150,000 increases the likelihood of malaria by 12-15 times. Various other studies have also found thrombocytopenia to be commonly associated with malaria[12],[13] which resolves after therapy.[14] The suggested mechanisms for thrombocytopenia include disseminated intravascular coagulation, or excessive removal of platelets by reticulo-endothelial system.[15] Anti-Platelet IgG has also been implicated in the pathogenesis of thrombocytopenia.[16] Thrombocytopenic malaria, in contrast to the non-thrombocytopenic variety correlates with a higher degree of parasitemia and increased cytokine production.[17] The pathogenesis of anemia in malaria is multifactorial. A complex chain of pathogenetic processes involving mechanical destruction of parasitized RBC′s, marrow suppression, ineffective erythropoiesis and accelerated immune destruction of nonparasitized RBC′s have been implicated.[18] Thrombocytopenia is a common observation in falciparum malaria with spontaneous recovery on treatment.. Both leukopenia[9]and leukocytosis[19] have been described in malaria. Increased red cell population dispersions or red cell distribution width (RDW) has been observed in malaria, and has been attributed to the red cell response to malarial parasite, and correlated with the degree of macrocytosis.[20] We included all consecutive cases of acute febrile illness in the study, and index test and gold standard were performed in all study patients in a blinded fashion. There have been two important limitations, firstly the spectrum bias of a referral hospital could have contributed to more severe cases being included in the study. This could have resulted in a greater proportion of patients with thrombocytopema in our study, as compared to the patients who would present to the primary care physicians. Secondly most patients receive empirical anti-malanal treatment prior to hospitalization, which could be responsible for a greater proportion of false negatives in our study. Clearance of parasitemia, as well as resolution of thrombocytopenia could have occurred after therapy in them. Other confounding factors for thrombocytopenia in acute fevers are sepsis and viral fevers, but a strong association of platelet count less than 150,000 in patients with slide positive malaria, as compared to the others argues for recognition of thrombocytopenia as an important parameter which may be associated with malaria, its complications an even response to therapy. Larger studies should be undertaken to establish its role as an indicator of response to threpy. CONCLUSION Presence of thrombocytopenia in a patient with acute febrile illness in the tropics increases the probability of malaria. This may be used in addition to the clinical and microscopic parameters to heighten the suspicion of this disease, and prompt initiation of the therapy. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04043t1.jpg] [ms04043t3.jpg] [ms04043t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}