 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
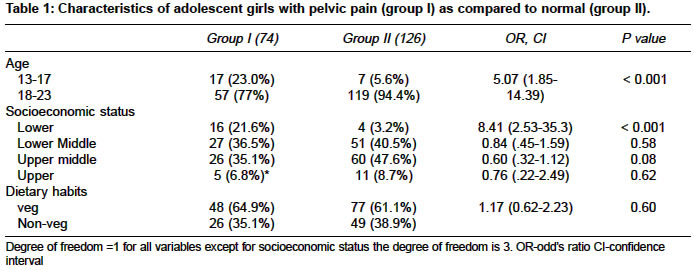
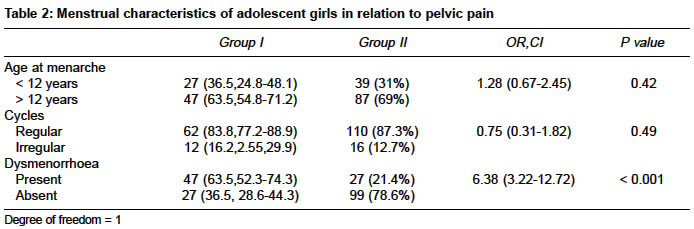
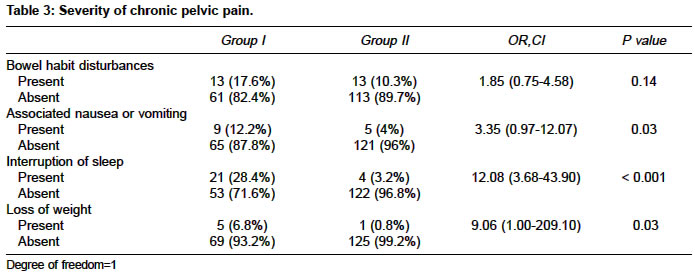
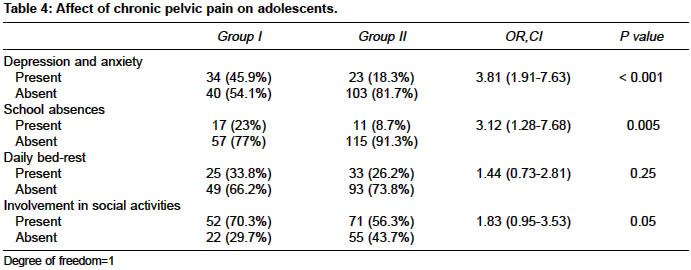
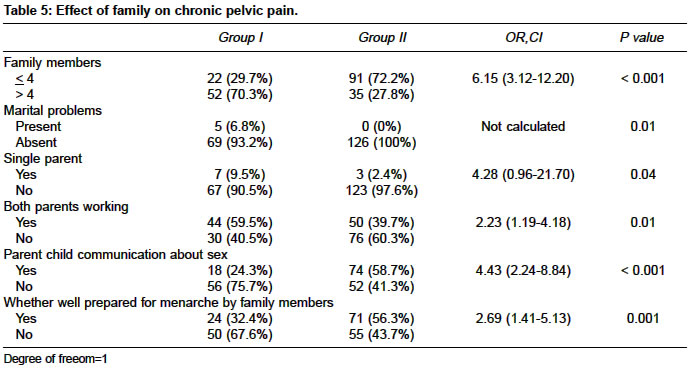
Indian Journal of Medical Sciences, Vol. 58, No. 7, July, 2004, pp. 275-282 Original Article Severity, affect, family and environment (safe) approach to evaluate chronic pelvic pain in adolescent girls Wadhwa Leena , Sharma JB, Arora R, Malhotra M, Sharma S Deptt. of Obstetric and Gynecology, Maulana Azad Medical College, Associated Lok Nayak Hospital, New Delhi - 110002 Code Number: ms04050 ABSTRACT BACKGROUND: Pelvic pain is common in adolescent girls in day-to-day practice. Severity, Affect, Family and Environment (SAFE) is a recent interview strategy to approach these patients and their families.. AIM: 1. To find the prevalence of pelvic pain in adolescent girls. 2. To find out the feasibility and acceptability of 'SAFE' approach in evaluating chronic pelvic pain in adolescent girls. SETTINGS & DESIGN: 200 adolescent girls aged 13-23 years were selected at random from school and colleges nearby hospital campus. METHOD: A questionnaire method was adopted. Adolescent girls selected were divided into two groups, group I (with pain) and group II (without pain). STATISTICAL ANALYSIS: It was performed using chi-square and Fischer tests with significance of p value being taken at 0.05. RESULTS: Out of 200 adolescent girls selected for interview, prevalence of pelvic pain was found to be 37.0%. Dysmenorrhoea was also found to have significant relationship with pelvic pain. Depression and anxiety, school absences and loss of weight were found to have significant association with pain. Pelvic pain was found to be more in adolescent girls with large family size (> 4 members), single parent, both parents working, ongoing marital problems at home and was less reported when there was good parent - child communication about sex and when the teenager was well prepared for menarche by the parents and the association with the above mentioned factors was found to be significant. CONCLUSION: 'SAFE' approach contributes in identifying health problems in adolescent girls with chronic pelvic pain.INTRODUCTION Pelvic pain is common in adolescent girls in day-to-day practice and because of multiple reasons is quite difficult to assess and manage. Chronic pelvic pain is not a disease, but a syndrome that results from a complex interaction between neurologic, muscloskeletal and endocrine systems that is further influenced by behavior and psychologic factors.[1] An understanding of the physical, cognitive and environmental factors associated with the pain are essential.[2] For the young patient who presents with chronic pelvic pain (CPP), a multidisciplinary approach is essential to facilitate diagnosis and management. Chronic pelvic pain is typically defined as cyclic or non-cyclic, intermediate or constant of at least six months duration primarily located in the pelvis and is severe enough to cause functional disability and require medical or surgical treatment. The approach to the patients with chronic pelvic pain should focus not only on organic causes of pain but simultaneously should also evaluate psychosocial and environmental factors related to pelvic pain. Psychologic concerns are an integral component of the evaluation and management of chronic pelvic pain.[3] Severity, Affect, Family and Environment (SAFE) is a recent interview strategy devised to approach these patients and their families. It includes discussion and assessment of emotional issues, psychosocial and environment factors. ′SAFE′ contributes in identifying health problems in adolescent girls. By the end of ′SAFE′ interview, the gynecologist will be able to evaluate the severity of symptoms, the degree to which serious pathology may be present, the role of contributing environmental factors including secondary gain and family issues. This strategy simultaneously evaluates medical and psychologic concern in adolescent girls and provides the gynecologist with a framework to guide further management.[4] The purpose of this study was to determine the feasibility and acceptability of SAFE approach in evaluating adolescent girls with chronic pelvic pain. MATERIAL AND METHODS This was a cross sectional study performed over one year between Sept 2002-Aug 2003. Out of 3 schools and 2 colleges a list of 600 girls between age groups 13-23 was prepared. A table of random number was generated from computer using the statistical software epistat. A random sample without replacement of 200 girls was selected through random number tables. Socioeconomic status was defined using kuppuswamy criteria. A pilot study conducted on 50 school or college adolescent girls revealed that 15% of the girls were having pelvic pain. The sample size was calculated by taking prevalence rate 15% with precision as 5%. The estimated sample size worked out to be 195. Thus it was proposed to enroll 200 patients in the study. A questionnaire method was adopted. The subjects were interviewed in detail and divided into two groups, patients with pelvic pain (group I) and another normal group without pelvic pain (group II) as control. Adolescent girls who experienced chronic pelvic pain of at least six months duration were included in the study. Verbal informed consent was taken from all the patients and the departmental ethical committee approved the study. Prevalence of pelvic pain as well as efficacy of ′SAFE′ approach in evaluating patient′s with chronic pelvic pain was studied. Severity of pelvic pain, affect on adolescent and role of family and environmental factors was assessed in patients with pelvic pain as compared to normal (group II) and the details of this SAFE approach questionnaire has been incorporated in form of [Table - 1], [Table - 2], [Table - 3], [Table - 4], [Table - 5] to provide the results. Severity of CPP was judged by various parameters as loss of weight, sleep and bowel habit disturbances. In addition to assessing pain severity, location, frequency, duration of pain, situations that make pain better or worse and its relation to menses were evaluated. If there is loss of weight in absence of deliberate dieting it was taken as non-physiological. If the adolescent is not able to have a consolidated sleep episode of 7 to 8 hrs per night, then it was taken as sleep disturbances. Bowel habit disturbances was taken as occurrence of diarrhea or constipation in an adult with previously regular habits, esp. when accompanied by systemic symptoms such as weight loss abdominal pain etc. (Harrisons). The next step is assessment of affect on adolescent due to pain, which may be in form of depression and anxiety, regular school absences, daily bed rest or social activities at bedside. Next to be considered in context of pain are family issues like family members, single parents, both parents working, ongoing marital problems, parent-child communication esp. about sex and many such factors due to which the adolescent wants to seek attention. Evaluation of patient′s environmental stressors in relation to pain is also important. Statistical analysis RESULTS The characteristic of adolescent girls with pelvic pain (group I) as compared with normal (group II) are given in [Table - 1]. There was significant relationship of pelvic pain with age and socio-economic status. It was found that there was more pelvic pain in adolescent girls after 18 years of age (77%, OR=5.07,CI 1.85-14.39). Girls with pain (36.5%, OR=0.84,CI .45-1.59) were more commonly found in the lower middle class whereas those without pain (47.6%, OR=0.60,CI .32-1.12) belonged to upper middle class. There was non-significant association of dietary habits with pain. The menstrual characteristics in both groups are depicted in [Table - 2]. There was non-significant association of age of menarche and regularity of menstrual cycles with pain whereas dysmenorrhoea was found to have significant relationship with pelvic pain. It was present in 63.5% girls in-group I as compared to 21.4% in-group II (OR=6.38,CI 3.22-12.72). [Table - 3] shows severity of pain as judged by bowel habit disturbances, associated nausea or vomiting, sleep interruption and loss of weight. Except for bowel habit disturbances which bears a non-significant association with pelvic pain, the other factors have significant association with pain and were more common in group I girls as compared to group II. The affect of pain on adolescent girls is shown in [Table - 4]. Depression and anxiety, school absences were found to have significant relationship with pelvic pain and were more common in group I girls whereas daily bed rest in association with pain has insignificant relationship. Involvement in social activities in spite of pain was more common in group I girls but the relationship is not significant. [Table - 5] shows effect of family on chronic pelvic pain. As compared to group II patients adolescent girls who suffered from pelvic pain (group I) had larger family size (> 4), increased marital problems at home, single parent and both parents working and the association was significant. When the teenager was well prepared for menarche by the parents and there was good parent-child communication about sex, pelvic pain was found to be less in group I adolescent girls and the association with these factors was found to be significant. DISCUSSION Chronic pelvic pain is a source of frustration to both the physician and the patient. The differentiation of psychogenic from organic pain in a busy gynecological clinic presents practical problems, with the added difficulty of knowing when to start and stop investigations.[5] Physicians have been ill equipped by their training to confront the multifaceted nature of the complaints of patients with chronic pelvic pain. In recent years, the emphasis in the clinical management has tended towards psychosocial or psychosexual involvement after organic disease has been excluded.[6] Most investigations are invasive, expensive and usually negative. A recent randomized prospective trial by peters and co-workers concluded that equal attention to both organic and other causative factors from the beginning of therapy is more likely to result in a reduction of pelvic pain than is a standard approach. [7] In our study primary outcome measured was prevalence of pelvic pain, which was found to be 37.0%. It was located in lower abdomen in 60.8% and both upper and lower abdomen in 39.2% cases. It lasted for < 24 months in 64.9% cases. It was related with menses in 75.7% cases. Frequency of pain was found to be once in a month in 59.4% cases, twice/month in 25.7%, and more than 3 episodes/month in 14.9% cases. Medication was taken by 23% of patients and pain was relieved with rest in 28.4% and no treatment was taken by 48.6%. Further diagnostic tests were done in only 8.1% cases. The secondary outcomes measured were;
Stones RW, Selfe SA et al (2000) reported that the affect of chronic pelvic pain is reflected in mood disturbances, disruption of normal activity and relationships.[8] Assessment of coping style is important as well as ascertaining information about any recent major life changes.[9] Depression and anxiety, interruption of sleep, weight loss points more toward organic cause of pain. This relationship was found to be significant in our study. Involvement in social activities in spite of pain points more towards functional cause of pain. An adolescent girl who reports discomfort and pain with menses that results in frequent and early departure from school but who still maintains an active social life (talking in the telephone, weekend dates) must be considered differently from a teen who is frequently absent from school and who does not communicate with peers.[4] The prevalence of pelvic pain was found to be more common with large family (> 4 members), single parent, both parents working or ongoing marital problems at home and other disturbed family environment. It is because teenager wants to seek attention. The clinician should determine what benefit, if any, the teen or a family member is receiving as a result of these somatic complaints. The diversion of a parent′s attention to a sick teen may provide a distraction from ongoing marital problems or work-related stressors. The gynecologist must assess the family′s make-up and environment. Pelvic pain was less commonly reported when there was good parent-child communication about sex and when the teenage was well prepared for menarche by the parents. It is also important to evaluate patient′s environment (peer, school and community) while approa-ching the adolescent girls with pelvic pain. Pelvic pain in adolescents is a common and frequently puzzling problem with many possible causes. Developing a treatment team, recognizing psychosocial and environmental factors and encouraging long term relationships are critical components in the care of these patients and in the prevention of recurrent symptom formation and future disability.[10] The ′SAFE′ approach allows the busy practitioner in identifying health problems in adolescent girls and provides the gynecologist with a framework to guide the physical examination, diagnostic procedures and further management including proper referrals of these patients. Use of this approach will minimize the need of invasive investigations and surgical procedures and simultaneously make the treatment therapy more effective. Identification of psychosocial factors related to pelvic pain helps in preventing pain exacerbations and improving quality of life. Strength of the study was that it was a study done at source, i.e. school or college and not on girls visiting hospitals. So it describes the realistic prevalence of the problem. The limitation of this study was that it was a small study done only on 200 girls and randomization was done only by the presence or absence of pain, which may be affected by the recall bias as many girls may have forgotten an attack of paln in recent part. ′SAFE′ approach contributes in identifying health problems in adolescent girls. Family and environment plays an important part in reducing the prevalence of pelvic pain. Identification of psychosocial factors related to pelvic pain helps in preventing pain exacerbations and improving quality of life. However, this study concludes that when a clinician does not have a direction of how to investigate and treat these difficult young girls, there is a systemic and scientific questionnaire that can be validly and scientifically used to better diagnose their condition and better manage them. As the present study highlights the importance of SAFE approach to manage these girls, and that psychomatic factors play a great role in some of them, it′s advisable to scientifically investigate these girls for any organic cause and to take psychiatric help in some cases. Increased awareness of its cost and impact on quality of life should promote increased medical attention to this problem.[11] Further studies to confirm these observations are needed, together with full reporting of those studies, which have been undertaken. Large multicentric double blind randomized studies are recommended to validate the routine use of SAFE approach to manage the adolescent girls with chronic pelvic pain. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04050t2.jpg] [ms04050t3.jpg] [ms04050t4.jpg] [ms04050t1.jpg] [ms04050t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}