 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
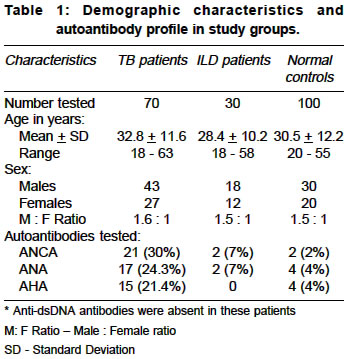
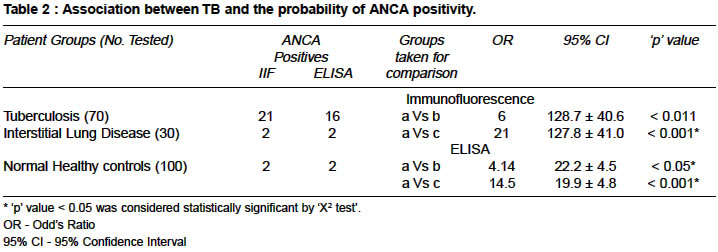
Indian Journal of Medical Sciences, Vol. 58, No. 7, July, 2004, pp. 283-288 Original Article Spectrum of anti-neutrophil cytoplasmic antibodies in patients with pulmonary tuberculosis overlaps with that of Wegener's granulomatosis Pradhan Vandana D, Badakere Suresh S, Ghosh Kanjaksha , Pawar Aruna R Institute of Immunohaematology, Indian Council of Medical Research, 13th floor, K.E.M. Hospital, Parel, Mumbai - 400 012 Code Number: ms04051 ABSTRACT BACKGROUND AND OBJECTIVES: Mycobacterial infections are known to induce the development of autoantibodies and a few of these antibodies are also known to be diagnostic markers for some other diseases and it is uncertain whether these autoantibodies play a role in the pathogenesis of autoimmune disorders. This study was undertaken to determine the prevalence of autoantibodies like anti-neutrophil cytoplasmic antibodies (ANCA), anti-nuclear antibodies (ANA), anti-double stranded antibodies (anti-dsDNA) and anti-histone antibodies (AHA)in pulmonary Tuberculosis. MATERIALS & METHODS: Seventy consecutive pulmonary TB patients, 30 patients of interstitial lung disease and 100 normal individuals were studied. ANCA and ANA were detected by indirect immunofluorescence test (IIF). Anti-dsDNA and AHA were tested by ELISA. RESULTS: ANCA was detected in 30% cases, and of these 52.4% showed perinuclear pattern (p-ANCA), 38.1% cytoplasmic (c-ANCA) and 9.5% showed an 'atypical' pattern. ANCA specificities by ELISA revealed that, 47.6% had anti-Myeloperoxidase (anti-MPO), 28.6% had anti-Proteinase3 (anti-PR3) and 19.1% had anti-Lactoferrin (anti-LF) antibodies. ANA and AHA were present in 24.3% and 21.4% cases respectively whereas anti-ds DNA antibodies were absent. Normal controls showed 4% and 2% positivity for ANA and ANCA whereas disease control group of ILD showed 7% of ANA and ANCA posititivy. CONCLUSION: The presence of autoantibodies in TB patients could have a multifactorial etiology. Clinically relevant is the presence of anti-PR3 antibodies. This finding along with pulmonary and renal manifestations could lead to a false diagnosis of Wegener's granulomatosis or vice versa because these autoantibodies may be present in both diseases. Tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis and is a scourge in the developing countries. TB is also prevalent in the black population of South Africa.[1] In India, a high prevalence of TB is due to the low socioeconomic levels and poverty.[2] The role of neutrophils in the pathophysiology of TB seems minor as compared to macrophages and remains uncertain but earlier reports have suggested that mycobacterial infections may play a role in the pathogenesis of autoimmune disorders.[3] Anti-neutrophil cytoplasmic antibodies (ANCA) are known to be highly diagnostic for ′pauci-immune′ small vessel vasculitis associated disorders like Wegener′s granulomatosis (WG), Microscopic polyangitiis (MPA) and Churg Strauss Syndrome (CSS). There are two main ANCA target antigens in these disorders namely, Myeloperoxidase (MPO) and Proteinase3 (PR3), which have diagnostic utility, though other cytoplasmic antigens like Lactoferrin (LF), Cathepsin G (CG), Elastase and Azurocidin are being investigated as possible targets for antibody mediated tissue destruction leading to vasculitis. Indirect immunofluorescence test (IIF) is a good screening assay for identifying ANCA positivity while enzyme linked immunosorbent assays (ELISAs) are used for identifying specificity.[4],[5] It is also found that mycobacterial infections are associated with induction of autoantibodies.[6] Tuberculosis is also known to be associated with vasculitis in a subset of patients. It is not very well known whether that vasculitis (endarteritis) is also driven by certain autoantibodies like ANCA. There is paucity of literature in the incidence and patterns of ANCA in florid cases of pulmonary tuberculosis. In addition pulmonary infiltration associated with haemoptysis in pulmonary tuberculosis may be mistaken as Wegener′s granulomatosis in non endemic areas if it is associated with high levels of ANCA positivity. The purpose of this study was to determine the prevalence of various ANCAs, their specificities and as it is known that there are some similarities between TB and ANCA associated vasculitis (AAV) i.e. pulmonary infiltrate, haemoptysis, systemic symptoms etc. Prevalence of other autoantibodies such as ANA, anti-dsDNA and AHA were also noted in these patients. MATERIAL AND METHODS In this study 70 consecutive pulmonary TB patients along with 100 age and sex matched healthy normal individuals were included. Sera of all 70 hospitalized patients were collected from a local TB hospital over a period of four months. Patients below 18 years of age and pregnant women were excluded from the study. All the patients with pulmonary TB had pulmonary infiltrate on X ray chest, AFB positivity in sputum or gastric aspirate and all of them presented with haemoptysis, 47/70 also had low grade fever with anorexia. Mantoux test was positive in all. Thirty patients with interstitial lung disease (ILD) were also taken as disease controls. In India TB is often diagnosed on the basis of interstitial shadow on X ray chest coupled with low grade fever, cough, anorexia and raised erythrocyte sedimentation rate (ESR). ILD was confirmed by combination of pulmonary function test including DLCo, bronchoscopy and bronchoalveolar lavage (BAL), high resolution spiral CT scan and consecutive three negative sputum test for acid fast bacilli (AFB) and negative BAL for AFB stain. As HIV infection is not an uncommon associate of TB in our country all the patients were tested for HIV after proper counseling and HIV positive patients were excluded. This prospective study was carried out after obtaining the requisite Ethics committee permission and informed consents from patients. Patients′ selection bias was avoided by selecting cases only after diagnosed by clinicians and the blinding was achieved as they were unaware of the laboratory findings. ANCA were detected using human neutrophils (PMN) by IIF technique which is considered as a ′gold standard′ for ANCA screening. Briefly, the method is as follows. PMN were used to prepare a cytospun substrate using Hettich Universal 16A cytocentrifuge and some slides were fixed with 96% ethanol and others with 0.45% formalin. After reacting with patient′s sera at 1:20 dilution, the slides were probed using FITC tagged polyvalent anti-human globulin serum and observed under a fluorescent microscope, Nikon, Optiphot II, Japan. Microphotography was also done using an automated photography system, Nikon AFX II A, Japan. The slides were also examined using a Confocal Laser Scanning Microscope, LSM 510, Carl Zeiss, Jena, Austria to visualize in greater detail and for clarity of the patterns of immunofluorescence.[7],[8] The specificity of the antibodies were further identified by antigen binding ELISAs for anti-myeloperoxidase (anti-MPO) and anti-Proteinase3 (anti-PR3) kits (Genesis, UK). A value <3.0u/ml was negative.3-5 u/ml was equivocal and >5u/ml were considered as positive. Anti-Lactoferrin (anti-LF) ELISA was developed using purified LF (Sigma, USA) as per the method described by Chikazawa et al,[9],[10] Anti-nuclear antibodies (ANA) were qualitatively and quantitatively tested by IIF[11] at 1:20 dilution of test serum, using HEp-2 cells obtained from Entero Virus Research Centre, Indian Council of Medical Research, Mumbai and cells were maintained in a continuous culture and harvested at log phase of growth. The results were interpreted in terms of titers i.e, test sera showing immunofluorescence at its highest dilution. Anti-dsDNAantibodies[12] and anti-histone antibodies (AHA) were detected by ELISA.[13] To study the association between TB cases and the probability of having ANCA positivity, Odd′s ratio (OR) was used. ANCA serology by IIF and ELISA in TB patients were statistically correlated with ILD patients and the normal healthy controls. Statistical significance was tested by Pearson′s ′X2 test′ with Yate′s correction and calculation of the 95% confidence intervals. A ′ p value′ less than 0.05 was considered statistically significant. RESULTS In this study 70 patients of pulmonary Tuberculosis were tested for ANCA, ANA and AHA along with a disease control group of 30 ILD patients and 100 normal controls. The age group was ranging between 15-63 years in TB cases and 18-58 years in ILD cases [Table - 1] and there was a slight male preponderance noted with M : F ratio of 1.6: 1 in TB cases and 1.5: 1 in disease and normal control groups. The overall incidence of ANCA was 30% in TB patients while ANA and AHA positivity was 24.3% and 21.4% respectively. ILD patients showed 7% positivity for ANCA and ANA whereas AHA were absent in them. Normal control group showed 2% positivity for ANCA and 4% positivity for ANA and AHA. [Table - 2] shows the statistical details of association between TB and the probability of ANCA positivity. ANCA studies revealed a total incidence of 30% positivity among TB patients studied (21/70). Of these 11 patients (52.4%) showed perinuclear (p-ANCA) immunofluorescence pattern and 8 patients (38.1%) showed a cytoplasmic (c-ANCA) pattern and two patients (9.5%) showed an ′atypical′ ANCA pattern. The normal control group showed 2% positivity for ANCA in low titers (1: 20) and only two ILD patients (7%) with 1: 40 titer value had ANCA. ANCA specificity by ELISA showed presence of anti-MPO antibodies in 10/21 patients (47.6%), anti-PR3 antibodies in 6/21 patients (28.6%) and anti-LF antibodies in 4/21 patients (19.1%). All the sera positive by ELISA were also positive in IIF test and a good correlation was found between IIF titers and ELISA values. It was seen that out of 11 patients that showed p-ANCA pattern on IIF where the titers varied between 1: 40- 1: 160 , 10 patients had anti-MPO antibodies having ELISA values ranging between 10-30 u/ml. Of the 8 patients that showed c-ANCA IIF pattern with 1: 40 to 1: 320 titer values, 6 patients had anti-PR3 antibodies where ELISA values varied between 8 to 25 u/ml. Both the patients that showed ′atypical′ or X-ANCA had anti-LF antibodies. The IIF patterns of ANCA positivity were compared with that of Wegener′s granulomatosis patients reported in the literature[4],[5] and from our own cases.[18] The overall incidence of ANA was 24.3% where 17/70 patients had ANA and AHA were found in 15/70 patients(21.4%). Incidence of ANA and AHA was slightly high in TB with renal manifestations as compared to TB having only pulmonary manifestations where 28/70 (40%) of patients also had additional symptoms of proteinuria, microscopic hematuria and/or raised Creatinine levels (> 2mg/dl). There was no correlation between development of autoantibodies and dosage or duration of therapy. Most of the patients were on standard anti-tuberculoid treatment i..e. Rifampicin, Isoniazid and Ethambutol. It was also observed that out of 17 ANA positive patients, 7 had both ANA and AHA whereas anti-dsDNA antibodies were absent. Control group showed 4% and 2% positivity for ANA and AHA respectively. DISCUSSION In India, Tuberculosis (TB) still remains one of the major causes of morbidity. Presence of autoantibodies have been reported in patients with mycobacterial infection like TB and leprosy[14],[15],[16],[17] The presence of autoantibodies like ANCA, ANA and AHA in TB patients is an interesting finding which makes us wonder whether the mycobacterial infection act as a trigger or if it is due to the drug regimen. Also in our study on another mycobacterial disease like leprosy ANCA positivity has been reported.[15] Rapoport et al, has reported the presence of ANA in TB cases having an increased ANA positivity in these patients mainly receiving Isoniazid treatment, where ANA positivity was further correlated with duration of the treatment.[1] However literature survey did not show INH induced ANCA positivity. In this study also INH induced ANCA can be ruled out as the incidence of ANCA positivity in untreated and treated cases was not much different or statistically significant. ANCA positivity by IIF should further be confirmed by ELISA for individual specificities and also Confocal Laser Scanning microscopy could give the true positivity especially in the cases where ANA is also positive. It is observed that p-ANCA positivity with corresponding anti-MPO specificity is commonly encountered in TB cases, but there could also be a small group of patients having Wegener′s granulomatosis, either in its limited or classical form and ANCA detection, showing c-ANCA pattern and presence of anti-PR3 antibodies in them would surely help in early and proper diagnosis. Tuberculosis may mimic many diseases including Wegener′s granulomatosis (a ′pauci-immune′ vasculitis). ANCA is an important serologic finding used to diagnose Wegener′s granulomatosis in association with relevant clinical and histopathological data. Hence findings of ANCA positivity in TB patients may confound the diagnosis of Wegener′s granulomatosis as many of the clinical features of this disease eg. haemoptysis, pulmonary infiltrate, hematuria, increased Creatinine may also be found in patients with tuberculosis. Infact we undertook this study mainly because four patients of Wegener′s granulomatosis at our Centre were mistakenly treated for pulmonary TB for a few months and Wegener′s granulomatosis was diagnosed when the patients fail to respond to anti-tuberculoid drugs.[18] Similar findings have been reported by others from this country.[19] ACKNOWLEDGMENTS We are grateful to DG, Indian Council of Medical Research (I.C.M.R.) and Director, Institute of Immunohaematology for facilities provided to us to carry out this work and Director, Entero Virus Research Centre (I.C.M.R.) for providing us with HEp-2 cell lines. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04051t2.jpg] [ms04051t1.jpg] |
| |||||||||

{kind=link}
{kind=link}