 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
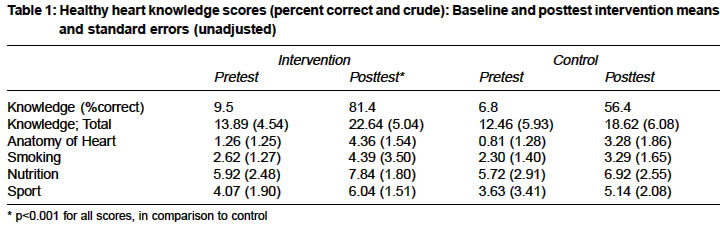
Indian Journal of Medical Sciences, Vol. 58, No. 7, July, 2004, pp. 289-296 Original Article A school-based intervention to teach 3-4 grades children about healthy heart; The persian gulf healthy heart project Nabipour Iraj , Imami Syed Reza , Mohammadi Mohammad Mehdi , Heidari Gholamreza , Bahramian Fatemeh , Azizi Fatemeh , Khosravizadegan Zahra , Pazoki Raha , Soltanian Ali-Reza , Ramazanzadeh Mahbobeh , Emadi Abdolresoul , Arab Jahfar , Larijani Bagher Persian Gulf Health Research Center, Bushehr University of Medical Science, Bushehr, I.R Code Number: ms04052 ABSTRACT BACKGROUND: Cardiovascular health promotion in children has the potential to reduce the risk of atherosclerosis in both the individual child and the population at large. It thus seems eminently reasonable to initiate healthful lifestyle training in childhood to promote improved cardiovascular health in adult life. AIMS: To test the hypothesis that a year long, classroom-based education for the third and fourth graders could change their knowledge scores about healthy heart. SETTINGS AND DESIGN: A randomized, controlled trial in elementary schools of Bushehr/Iran. METHODS AND MATERIALS: A total of 14 elementary schools, categorized by socioeconomic types and male and female setting were selected and randomized into control or intervention groups. Subjects were 1128 third and fourth graders, aged 9 to 10 years (49.1% boys and 50.9% girls). Over a course of 8 weeks, health educators and sport teachers of the elementary schools presented two hours sessions per week on heart function, nutrition, and exercise for healthy heart and living tobacco free for the intervention group. The education program was based on HeartPower! Program, an American Heart Association program. STATISTICAL ANALYSIS: Mann-Whitney U test and Wilcoxon matched-pairs signed rank test and Bonferroni correction for the two pair wise comparisons were used. RESULTS: Total heart knowledge at posttest was 25% correct higher in the intervention than in the control group (p<0.001). Difference in means of total healthy heart knowledge scores between control and intervention group increased from 1.43 points in baseline to 4.02 points in posttest (p<0.001). CONCLUSION: It can be concluded that the classroom-based cardiovascular health promotion had a significant effect on the heart healthy knowledge. Therefore, schools provide an excellent setting for introducing comprehensive healthy heart education and promotion of cardiovascular health to the general population.INTRODUCTION The process of atherosclerosis may begin developing during childhood[1]. It is based partly on evidence of fatty streaks and atherosclerotic lesions that have been found at postmortem in the aorta and coronary arteries of 6- to 30-year-olds; these were related to antemortem cardiovascular disease risk factors such as smoking, elevated serum cholesterol, and high body mass index.[2],[3],[4],[5],[6] It thus seems eminently reasonable to initiate healthful lifestyle training in childhood to promote improved cardiovascular health in adult life.[7] A growing number of children attend elementary through high school, the schools are an especially effective and efficient system for providing health education for children. Both classroom-based and risk-based interventions had positive effects on physical activity and knowledge, with trends towards reduced body fat and cholesterol in elementary school children; however, the results from the large-group, classroom-based approach showed stronger trends and were much easier to implement in the school system.[8],[9] The few large-scale randomized, controlled studies of school-based programs to reduce cardiovascular risk in children have early results.[9],[10],[11],[12],[13] Most school-based interventions included interactive instruction on selected topics related to heart disease. Interventional time range from 1 full school day to 30-45 minutes a day once a week over an academic year. Sample sizes in these studies ranged from 90 to 2,973 children. Some studies showed improvement in knowledge; in some children, cholesterol levels were lowered.[8],[13] The major purpose of the school-based project of The Persian Gulf Healthy Heart Study, a controlled, randomized field trial, was to determine whether a school-based intervention could improve healthy heart knowledge in third- and fourth-grade children in Bushehr Port, a city along the Iranian coast of the Persian Gulf. MATERIALS AND METHODS This study tested the hypothesis that a year long, classroom-based education for the third and fourth graders could change knowledge scores about healthy heart from beginning to the end of the program in comparison to control group. The education program was based on HeartPower! Program.[14] HeartPower! is an American Heart Association program designed to encourage children to engage in heart healthy lifestyles. This project was conducted in Bushehr Port, the center of Bushehr Province, with a population of 150,000 and coronary events of 481.05 and 156.61 per 100,000 for men and women, respectively. The organization of elementary schools in I.R.Iran was categorized into three types according to financial supports; governmental, semi-governmental and private, in order of frequency. All financial support of governmental and a part of financial support of semi-governmental schools are provided by Ministry of Education, but private schools are free of financial support of government but their educational program follows the rules of Ministry of Education. These school types revealed socioeconomic status of the studied area, therefore the schools were randomly selected from these categories in order of their frequency in each cluster. There were no significant difference in type of schools and gender distribution between the selected subjects (14 schools) and the total schools of the city (with 104 elementary schools). Schools which were stratified by types (governmental, semi-governmental and private) and setting (girl and boy) were randomly assigned to intervention or control groups. According to Harrell and colleagues,[9] total estimate sample size was 1200 third and fourth graders, aged 9 to 10 years (600 children in intervention and the other half in control group). There were no significant difference in school type, gender distribution and third and fourth graders at the schools between the intervention and control groups. All children completed a 30-question healthy heart knowledge test as a baseline examination. It had four subscales including 7 questions for anatomy of heart (e.g., Which vessel carries blood away from the heart?), 6 questions for smoking as a risk factor for cardiovascular diseases (e.g., What is the relationship of smoking and hear diseases?), 8 questions for exercise (e.g., How much physical activity should you perform per day?), and 9 questions for healthy heart nutrition (e.g., How many servings of fruits and vegetables should you have every day?). The questions were multiple choice, matching and labeling types. Ordinarily, each elementary schools in Iran has a health educator and a sport teacher. Both the intervention and control groups received their regular education program from their health educators and sport teachers. But, over a course of 8 weeks, ordinary health educators and sport teachers of the primary schools presented 2 hours sessions per week on heart function, nutrition, physical activity and living tobacco free for the third and fourth graders at the intervention group. The education program was based on HeartPower! Program for grades 3 through 5.[14] Health educators and sport teachers of the intervention group received especial training for educating HeartPower! Program in a workshop. Health educators discussed heart function, circulation and oxygenation in anatomy session and emphasized the importance of food pyramids and managed group activity focusing on meal planning and encouraged importance of living tobacco-free and read stories about smoking and heart disease for the children. Sport educators discussed importance of exercise and engaged children in physical activities such as jumping jacks or running in place and planned aerobic activities in small-group games. All the students passed the second examination in healthy heart after the intervention, as posttest. Mann-Whitney U test was used to reveal to what extent did knowledge scores about healthy heart lifestyles change from beginning to the end of each program, and between intervention and control groups. Subscales of healthy heart knowledge scores for anatomy of heart, smoking, exercise and healthy nutrition were adjusted and compared for each subject by Friedman matched samples and Wilcoxon matched-pairs signed rank test. Bonferroni correction for the two pair wise comparisons was used. RESULTS The sample included 1128 children (49.1% boys and 50.9% girls) in third and fourth graders at the study schools. Half of the children were third grader (51.4%). There were no significant differences in baseline demographic characteristics of the intervention and control groups; including sex, grade (third or fourth) and socioeconomic status data. Of all children in the interventional group, 81.4% attained a passing score of 75% by the end of study, whereas 56.4% of children in the control group passed. In other words, total heart knowledge at posttest was 25% correct higher in the intervention than in control subjects (p<0.001). Difference in means of total healthy heart knowledge scores between control and intervention groups increased from 1.43 points in baseline to 4.02 points in posttest (p<0.001, [Table - 1]. There was no difference in total heart healthy knowledge according to gender or grader. The mean ranks for healthy heart knowledge subscales for nutrition, exercise, smoking and anatomy of heart in baseline were 3.36, 2.80, 2.49, 1.36; respectively (p<0.001). The mean ranks did not change in posttest, but knowledge in anatomy of heart increased significantly in posttest in intervention group (3.1 points versus 0.46; p<0.001). The same significant changes in the other healthy heart subscales were observed [Table - 1]. DISCUSSION This study tested an 8-week school-based intervention for third and fourth graders, in order to improve their healthy heart knowledge. The students who participated in the HeartPower! , a school-based educational program, showed improvement in their knowledge of healthy lifestyles. The physiological measures such as body mass index or serum cholesterol level were not evaluated in this study. Because, it may be unrealistic to expect dramatic physiological changes in a young population, given the level of intensity of a primary prevention program and the relatively healthy general population at which it is targeted. In fact, most population-based education studies that have reported on intervention effects on physiological variables have shown modest change or no change.[15],[16],[17] It could be due to short term studies which lacked of time needed to see these changes. However, children in the Cardiovascular Health in Children Study, a randomized, controlled field trial in 12 schools across North Carolina, had significantly greater knowledge (7.9% more correct) and a significant increase in self-reported physical activity than children in the control group. Trends for the intervention group were a reduction in total cholesterol level (-5.27 mg/dl), an increase in aerobic power, a reduction in body fat, and smaller rise in diastolic blood pressure than control children.[18] The Cardiovascular Health in Children intervention was more intense than the other studies, involving regular physical activity as well as health knowledge, which may explain these differences. As part of the other study, Child and Adolescent Trial for Cardiovascular Health, 4019 children from four states and representing multiple ethnic groups were measured for selected risk factors both at baseline and after 2&frac 12; years of intervention. Although the school-based program effected significant institutional changes in food service and physical activity behaviors, these did not translate to significant changes in risk factors at these ages. These behavioral changes, however, if sustained into adulthood, have the potential to influence cardiovascular risk reduction.[19] Overall, cardiovascular health promotion linked to healthy heart education for children has the potential to reduce the risk of atherosclerotic disease in both the individual child and the population at large.[7] Generally, two school-based interventions could be implemented in order to improve heart health in children; classroom-based intervention and risk-based approach on a subset of children with positive risk factors for cardiovascular diseases. Harrell and colleagues in the first large randomized, controlled study, compared these approaches. The study demonstrated that both the classroom-based approach and the risk-based approach can somewhat improve cardiovascular risk profiles in elementary school children. However, the results from the large-group, classroom-based approach showed stronger trends and were much easier to implement in the school system.[9] Our study was a classroom-based approach and it was practical because it based on programs readily available to schools and should not require additional teachers or expensive materials. Any qualified school health nurse and sport educator can teach its components for the healthy heart. However, the effective implementation of healthy heart education depends to a large extent on the training and motivation of teachers, administrators, and food service staff at the schools.[20],[21],[22],[23] The process of cardiovascular disease that begins early in life is possibly related to obesity, high serum cholesterol levels, and a diet high in total and saturated fat. Therefore, reducing the intake of foods high in fat and cholesterol early in childhood may delay or reduce the risk of cardiovascular disease later in life.[23] Because evidence linking higher blood cholesterol levels in children and adolescents with atherosclerotic lesions in coronary and other arteries is accumulating.[24],[25] The elementary schools are a suitable media to transfer knowledge of healthy nutrition for heart; in our intervention group, the mean rank was significantly higher for healthy heart nutrition than the other subscales for healthy heart knowledge in the posttest. It is important to note that childhood nutritional behaviors have a profound impact on future adult lifestyle choices. The original CATCH results demonstrated that school-level interventions could modify school lunch and school physical education programs as well as influence student behaviors. A 3-year follow-up of students who participated in CATCH study without further intervention suggested that the behavioral changes initiated during the elementary school years persisted to early adolescence for self-reported dietary and physical activity behaviors.[26] One of the subscale healthy heart knowledge for our intervention group was anatomy of the heart and circulation. The objective of the lesson was based on American Heart Association HeartPower! Program.[14] The students in post- intervention period were able to recite the anatomy of the heart, state that a healthy heart is a pump with valves allowing blood to flow in only one direction and distinguish between arteries and veins and describe the function of coronary arteries. The student painted heart in very primitive form before intervention; but during the intervention phase, the paints of heart changed to a more logic and anatomic ones. The most improvement in healthy heart knowledge score was for the anatomy of heart in interventional group (3.1 points, versus 2, 1.7, 1.9 for sport, nutrition and smoking; respectively). However there was significant difference between healthy lifestyle knowledge of intervention group and control subjects (p<0.001), but the knowledge scores of students in control group also increased in posttest, because the children were such young readers at baseline, we elected to overburden them with questionnaires at pretest. The children participating in this study looked forward to the healthy heart lessons and participated in them with enthusiasm. Therefore, programs specific for cardiovascular health are valuable supplements for schools and provide more in-depth education and skill-building in areas targeting reduction of cardiovascular risk. However, a short 8 weeks program will not be sufficient to reach all of the goals for prevention of cardiovascular disease. Further research and intervention needs to include the family and the media including food service industry, government and the community. We would suggest, however, that to produce long-term population effects, school-based interventions should be conducted at least annually throughout the elementary, middle, and even high school years. ACKNOWLEDGEMENT This project was supported by governmental grant from Tehran Endocrine Research Center, Tehran University of Medical Science, Tehran, I.R. Iran. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04052t1.jpg] |
| |||||||||

{kind=link}