 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
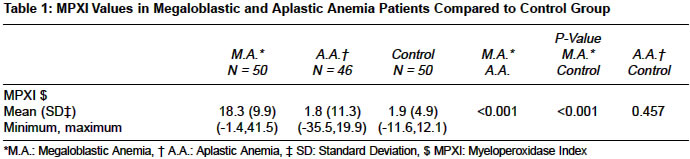
Indian Journal of Medical Sciences, Vol. 58, No. 8, Aug, 2004, pp. 345-348 Original Article Role of myeloperoxidase index in differentiation of megaloblastic and aplastic anemia Ziaei Jamal Eivazi, Dastgiri Saeed Hematology and Oncology Department, Imam Hospital, Tabriz Code Number: ms04061 ABSTRACT BACKGROUND: Elevated neutrophil myeloperoxidase may have a role in the diagnosis of megaloblastic erythropoiesis. AIMS: To study the differentiating role of myeloperoxidase index in megaloblastic and aplastic anemia. SETTINGS AND DESIGN: The myeloperoxidase index (MPXI) was studied in 96 patients with megaloblastic and aplastic anemia diagnosed on bone marrow aspiration and biopsy examinations. METHODS AND MATERIALS: MPXI was measured with Technicon H1 (Bayer) automated analyzer. Nonparametric Mann-Whitney statistical test was used to compare the MPXI values between groups. RESULTS: The mean MPXI in megaloblastics and aplastic anemia was 18.3 and 1.8 (p<0.001) respectively. MPXI >20 denoted megaloblastic and MPXI <-11.6 denoted aplastic anemia. CONCLUSION: MPXI measurement may assist differentiation of megaloblastic from aplastic anemia, while MPXI >20 rules out aplastic and MPXI <-11.6 rules out megaloblastic anemia. Keywords: Megaloblastic, aplastic, anemia, myeloperoxidase index INTRODUCTION Patients with pancytopenia and macrocytic red cell indices may pose a difficult diagnostic problem. The possible causes are numerous including megaloblastic and aplastic anemia.[1] Generally evaluation of these patients includes examination of peripheral blood smear and bone marrow specimens.[2],[3],[4] Recently, Taylor and Bain[2] have reported that an elevated neutrophil myeloperoxidase index (MPXI) may be indicative of a diagnosis of megaloblastic anemia. The biologic basis of elevated MPXI in patients with megaloblastic anemia is the presence of increased number of MPXI- laden granules in the neutrophils due to skipped cellular divisions during maturation. The MPXI can be measured by Technicon H1 (Bayer) automated cell counter.[3] Myeloperoxidase is a microbicidal protein, which exists in the primary granules of myeloid cells and takes part in the defense of the organism.[5],[6] It is synthesized in the promyelocyte where it is packed into azurophilic granules.METHODS AND MATERIALS The medical records of cases diagnosed as megaloblastic and aplastic anemia were studied from 1995-2003. Fifty cases of megaloblastic (35 males and 15 females) and 46 patients with aplastic anemia (31 males and 15 females) met the study criteria. The age range for megaloblastic and aplastic anemia was 12 to 72 and 12 to 50 years, respectively. As the control group, we selected 50 normal and healthy subjects (25 males and 25 females) with the age range of 12 to 50 years. Inclusion criteria for megaloblastic anemia patients included age > 12 years old, typical peripheral smear, bone marrow aspiration with trephine biopsy findings such as hypersegmented neutrophils, macro-ovalocytes and giant band cells who responded to treatment with vitamin B12, 2000 ug subcutaneously or intramuscularly and folic acid, 1-3 mg orally for six weeks. Exclusion criteria for megaloblastic patients were blood transfusion and cases with other diagnosis in trephine biopsy report such as megaloblastoid changes with myelodysplastic syndromes or aplastic anemia. Inclusion criterion for aplastic cases was bone marrow cellularity < 25 percent in trephine biopsy. We excluded patients who had blood transfusion, or had received chemotherapy or radiation therapy. Peripheral smear and bone marrow aspiration slides stained with May-Graunwald-Giemsa staining and trephine biopsies were stained with hematoxilin and eosin. Two hematologists reported peripheral smear and bone marrow slides and trephine biopsies were reported by an expert hematopathologist. They have contributed to the study and yet not included as authors. MPXI was assessed using the first complete blood count (CBC), performed by Technicon H1 (Bayer) instrument before transfusion or treatment. MPXI is a direct and routine reading parameter in the machine result with the normal range of -10 to +10. Peroxidase activity and cell size are measured by light absorbance and scatter as each leukocyte flows through a mercury arc light beam.[3] It is computed as follows: MPXI = Mean X of Sample Neutrophil- Mean X of Archetype Neutrophil / Mean of Archetype Neutrophil ×100. Mean of Sample Neutrophil. Is the average absorption chanel (X) observed for neutrophils in the sample. Mean of Archetype Neutrophil Is the average absorption channel (X) specified for the neutrophil cluster in the normal staining archetype.[7] The values below (-25) represent people with myeloperoxidase deficiency, an autosomal recessive anomaly.[8] Serum vitamin B12 and red cell folate levels were not determined. Non-parametric Mann-Whitney statistical test was used to compare the MPXI values between cases with megaloblastic and aplastic anemia, and control group. RESULTS In [Table - 1], patients with megaloblastic and aplastic anemia, and control subjects are compared in terms of minimum, maximum and mean values for the MPXI. The difference between the mean value of MPXI for megaloblastic anemia (18.3) and aplastic anemia (1.8) was statistically significant (P<0.001). The difference of the mean value of MPXI in megaloblastic anemia (18.3) and control group (1.9) was also statistically significant (P<0.001), while there was no significant difference in the mean value between aplastic (1.8) and control subjects (1.9), (P=0.46). DISCUSSION Differentiation of megaloblastic anemia from the other causes of macrocytosis requires the use of laboratory tests such as complete blood count, peripheral smear examination, and bone marrow specimen.[6],[9],[10] As aplastic anemia may be macrocytic in some patients; it must be differentiated from megaloblastic anemia.[11],[12] Determining of MPXI can be useful in differentiation between two groups of macrocytic anemia. In this study, we were interested in a simple test to differentiate between megaloblastic and aplastic anemia. Our study showed that the mean value of MPXI in megaloblastic anemia was significantly higher than aplastic anemia indicating that the measurement of MPXI, is a simple and useful test, in differentiation of these disorders. Several studies of elevated neutrophil myeloperoxidase in megaloblastic anemia have previously been reported.[13] They have not however indicated the role of MPXI in detecting aplastic anemia. According to this study, all MPXI values of less than -11.6 denoted aplastic anemia, while the values between -11.6 and -1.4 may be considered as aplastic, megaloblastic, or normal. MPXI values of less than -1.4 rules out megaloblastics, and MPXI greater than 20 will rule out aplastic anemia. Our study had some limitations: we did not determine vitamin B12 and folate levels in the study subjects, and the sample size was relatively small. We conclude that MPXI measurement is a helpful tool in differentiation of two macrocytic and pancytopenic anemias. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04061t1.jpg] |
| |||||||||

{kind=link}