 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
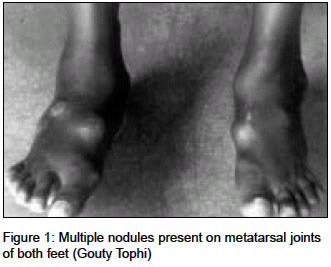
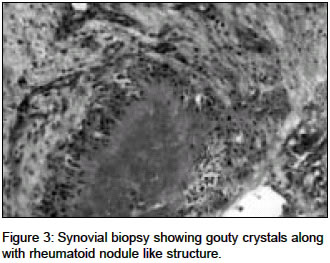
Indian Journal of Medical Sciences, Vol. 58, No. 8, Aug, 2004, pp. 349-352 Case Report Concomitant gout and rheumatoid arthritis - A case report Khosla Pooja, Gogia Atul, Agarwal PK, Pahuja Amit, Jain Sunil, Saxena KK Department of Medicine, Sir Ganga Ram Hospital, Rajinder Nagar, New Delhi - 110060 Code Number: ms04062 ABSTRACT We report a case of definite rheumatoid arthritis and co-existing gout. Although gout and rheumatoid arthritis are relatively common entities individually, the co-existence of these two conditions is rare. Keywords: Gout, Rheumatoid Arthritis INTRODUCTION Gout and rheumatoid arthritis rarely co-exist in the same patient. As separate disease entities they are relatively common. Rheumatoid arthritis affects 2-3% of the population[1] with a female to male ratio of 3:1, while gout affects 0.25% of the population, with 90% of the cases occurring in males.[1] It has been reported that there is a strong negative correlation between rheumatoid arthritis and gout.[2]CASE HISTORY A 55-year-old ex-army man was admitted with a 10-year history of pain in the ankle joints followed by involvement of left 1st metatarsophalangeal joint. He had asymmetrical joint pains and swelling at irregular intervals with exacerbations and remissions. The symptoms subsided in between but there was no period when patient was completely pain free. He did not have associated warmth and erythema although swelling and tenderness were present. Three years after onset of joint pains, patient started having pain in small joints of hands, knees, ankles, shoulders and elbows, with early morning stiffness lasting for more than four hours. Joint pains were incapacitating and he had to quit his job. Initially pain was localized to the ankles and left 1st metatarsophalangeal joint but gradually went on to involve the rest of the joints over the next 7 years or so. He consulted various practitioners and took allopathic and indigenous medications but to no relief. Two months prior to admission he presented with multiple nodular swellings on feet, hands, wrists and elbows. Patient′s past medical history is significant for hypertension, diabetes mellitus, chronic ethanolism and renal stones for which he underwent left nephrectomy about 25 years ago. Family history is non-contributory. On examination multiple nodules were present on metatarsal joints of both feet, Achilles tendon bilaterally, left prepatellar bursa, bilateral metacarpophalangeal joint, right olecranon process. There was swelling and tenderness of PIP and MCP joints of both feet. [Figure - 1] Laboratory data revealed hemoglobin - 8.9gm/dl, ESR 124 mm at the end of first hour, leucocyte count 7400/cmm with normal differential count. Random blood sugar was 139 mg/dl, Creatinine- 1.6 mg/dl; serum uric acid level was 10.9 mg/dl. His 24 hour urinary uric acid excretion was 446 mg/dl. Serum calcium, phosphorus, LFT, electrolytes and lipid profile were normal. Serum iron was 7 mg/dl, TIBC 244 mg/dl. Stool for occult blood was negative. Rheumatoid factor was 2560 iu/ml (by latex agglutination method) and CRP was 96 mg/dl. X-rays of both feet showed multiple lytic areas in 2nd and 3rd metatarsal and tarsal bones. X-rays of both elbows showed soft tissue swelling at olecranon process, right more than left. X-rays of both hands showed subarticular erosions at distal end of radius, ulna, scaphoid, radial aspect of 2nd and 3rd proximal interphalangeal joints bilaterally and left triquetrum with associated soft tissue swelling [Figure - 2]. X-ray of both knees revealed reduced tibio-femoral and patello-femoral joint space with subarticular lytic area, sclerosis and soft tissue swelling bilaterally right more than left. These findings were suggestive of gout lus rheumatoid arthritis. X-ray pelvis showed bilateral sacroiliitis. Sonography of the abdomen revealed mild hepatomegaly with grade I fatty changes with right kidney 12.4x4.6 cm in size. Thick chalky white fluid was aspirated from the nodular swelling at the right metatarsophalangeal joint. It was alkaline with numerous polymorphs, WBC 25000 cells/cmm, 90% polymorphs and 10% lymphocytes with monosodium urate crystals with birefringence. Patient underwent arthroscopy of the right knee and synovial biopsy was taken. Arthroscopic finding revealed synovial hypertrophy with gouty crystals embedded and spread everywhere in the joint. Synovial biopsy was compatible with gouty tophi in synovium along with rheumatoid nodule like structure [Figure - 3]. Diagnosis of chronic tophaceous gout with rheumatoid arthritis was made and the patient was started on colchicine, allopurinol and methotrexate. DISCUSSION The co-existence of gout and RA may be supported by both clinical and laboratory criteria.[3] Our patient had recurrent gouty attacks superimposed by rheumatoid arthritis. He had high serum uric acid; monosodium urate deposit in subcutaneous nodules, high titer of RF, radiographic changes of gout and erosive RA and histological evidence of a rheumatoid arthritis. These manifestations have been proposed as the criteria for the coexistence of both diseases.[4] A literature review revealed 17 patients with concomitant gout and RA.[3],[5] The difficulty of reaching a diagnosis of coexistence of both diseases may be due to the fact that it takes time to establish definite evidence of gout clinically as chronic tophaceous gout mimics rheumatoid arthritis, so a clinician does not suspect the condition. RA or their concurrence. Many features of gout during the evolution of the disease may mimic RA (We would like to tell that we are not talking about acute gout but it is chronic tophaceous gout and it has a similar course i.e. insidious and gradually progressive.) or vice versa. In all cases in which gout and RA were associated no difficulty was encountered in establishing the diagnosis of gout.[2] Papers in the literature clearly document the presence of gout but rely on the presence of morning stiffness, symmetrical synovitis and positive RF with low or high titer for the diagnosis of RA.[2] Morning stiffness and fusiform swelling of PIP and MCP joints, though suggestive of RA, are misleading since these findings can occur in polyarticular tophaceous gout. It has been reported that chronic synovitis in gout may also simulate RA when studied by means of arthrography.[2] The presence of lymphocytic infiltration with germinal centers and the absence of crystals in the chronic synovitis support the diagnosis of RA.[2] and a high incidence of positive test for RF has been reported in gout without clinical evidence of RA. Kozin and McCarty[1] found 30% of patient with chronic topahceous gout and 10% of patients with acute gout to have rheumatoid factor present in low titers (<1:320). Other researchers also found positive titers of RF, but in a smaller percentage of patients.[6] In our case, the pathological changes present, in the synovial membrane and the high titer of RF (1:2560) support the diagnosis of RA beyond doubt. Unusual feature observed in our patient was bilateral sacroilitis. This is an uncommon finding, seen in rheumatoid arthritis.[7] There is no clear data on Sacroilitis in gout but cases showing sacroilitis in gout have been reported (Reference: Talbott JH, Altman RD, Yu TF. Gouty arthritis masquerading as Rheumatoid arthritis. Seminars in Arthritis and Rheumatism 1978; 8(2): 100-101. We agree with Atdijian and Fernandez and Rizzoli et al[2],[6] that diagnosis of this coexistence can be made with certainty by finding the histological evidence of rheumatoid nodules and monosodium urate crystal deposition. Synovial biopsy from right knee in our patient had changes of gout and rheumatoid arthritis. The fixation of biopsy materials in alcohol is important since granulomas with histologic features resembling rheumatoid nodules or rheumatoid synovitis may show crystals of MSU when examined under contrast polarizing light microscope.[2] After a confirmed diagnosis, treatment with Disease modifying drugs along with hypouricemic therapy can be safely started. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04062f3.jpg] [ms04062f2.jpg] [ms04062f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}