 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
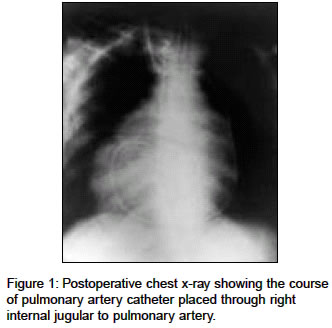
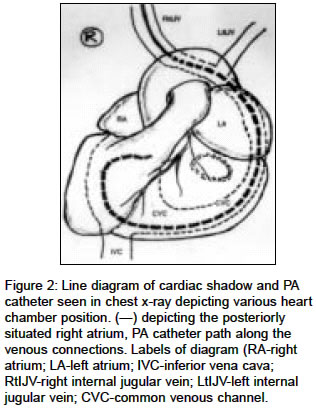
Indian Journal of Medical Sciences, Vol. 58, No. 8, Aug, 2004, pp. 353-356 Case Report Pulmonary artery catheter insertion in a patient of dextrocardia with anomalous venous connections Tripathi Mukesh, Kumar Naresh, Singh PrabhatK Department of Anaesthesiology and Critical Care Medicine, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow Code Number: ms04063 ABSTRACT In a young adult patient having situs solitus with dextrocardia the attempted pulmonary artery catheter placement for emergency mitral valve replacement required an unduly long length (50cm) of catheter insertion to get into right ventricle and then into pulmonary artery. Although catheter coiling was suspected initially, chest x-ray taken after successfully placement revealed an uncommon congenital anomalous venous connection i.e. right internal jugular opening into left sided superior vena cava then into inferior vena cava after running all along the left border of the heart. With the result, it required to pass 50cm of PA catheter to get into right ventricle in our patient. This emphasizes the need to look for abnormal venous connections during echocardiography and x-ray screening in congenital heart disease. Fluoroscopy is recommended when an unusual length of pulmonary artery catheter insertion is required to enter the pulmonary artery. Keywords: Pulmonary artery catheter, Dextrocardia, Congenital heart disease, Mitral valve replacement The flow-directed pulmonary artery (PA) catheter has revolutionized the hemodynamic monitoring during open-heart surgery and its use is advocated invariably in patients of severe pulmonary hypertension (PH) and essentially in emergency cardiac surgery. For its insertion, the right internal jugular vein is commonly selected, because of its straight and valve free course into right atrium. Passage of PA catheter from the site of vein puncture to the pulmonary artery is guided by, monitoring the changes in pressure waveform, on its course to right atrium, right ventricle, and pulmonary artery till the point of wedging of its tip. In average adult, PA catheter enters into right atrium approximately at 12-20 cm marks, in PA at 40-45 cm and usually wedges around 45-55 cm marks on PA catheter. As we could not find a similar clinical report in literature, we wish to report our unusual experience during pulmonary artery catheter insertion in a patient with dextrocardia and previously unrecognized anomalous venous connection. CASE REPORT A 37-year-old male patient with situs solitus and dextrocardia was also diagnosed to have severe mitral stenosis and pulmonary hypertension due to rheumatic heart disease. The patient developed severe mitral regurgitation during attempted balloon mitral valvotomy due to injury to mitral valve leaflet. This patient was taken up for emergency mitral valve replacement. Echocardiography revealed situs solitus, dextrocardia, mitral valve area of 0.6, thick and calcified mitral leaflets, and left atrial dilatation (55 mm). Left ventricle size was normal and had good contractility with ejection fraction of 68%. In post balloon valvotomy period, echocardiography showed severe mitral regurgitation with projected right ventricular systolic pressure of 60 mmHg. In the operation theater, continuous cardiac output measuring PA catheter (6Fr) was introduced through the introducer sheath (6Fr) placed aseptically into right internal jugular vein under local anesthesia. During insertion of pulmonary artery catheter, right atrial pressure trace was seen at 20 cm mark. However, even upto 45 cm mark, RA trace continued. Apprehending coiling of catheter in RA, catheter was withdrawn back to 20 cm mark and reinserted it with inflated balloon while monitoring pressure waveform. In the second attempt, it again failed to get into right ventricle even at 50 cm mark. Although coiling was considered but surprisingly cardiac arrhythmias were not seen during manipulation. At this point more experienced consultant took over for the PA catheter insertion and he could pass the catheter into right ventricle by passing it smoothly up to 55 cm mark. Waveform characteristic of its entry into pulmonary artery was seen at 65 cm mark and when its tip failed to wedge even at 70 cm mark, we fixed the catheter at this point without advancing it further, lest coiling or knotting occur. After mid sternotomy incision to open thorax, we observed that right atrium was on right side but rotated behind the right ventricle from normal. The right-sided superior vena cava was absent. Right internal jugular was opening into left sided superior vena cava to form a common venous channel running all along the left border of the heart to open into the inferior vena cava at the posterior and inferior surface of the heart and both opening into the right atrium single opening. The pulmonary artery catheter inserted through the right internal jugular vein went through the common venous channel formed by the two jugulars. The catheter inside the common venous channel traversed all along the left border of the heart, reached the inferior and posterior surface of the heart, and then coursed upwards to enter into the inferior vena cava, the right atrium, right ventricle and the pulmonary artery [Figure - 1], [Figure - 2]. Since the RA was posterior, itscannulation was difficult due to arrhythmia and hypotension. Venous drainage from pulmonary artery was secured for quick initiation of cardiopulmonary bypass and then inferior vena cava cannulation was performed. Postoperative chest x-ray confirmed the course of PA catheter [Figure - 1]. The patient had an uneventful postoperative period. DISCUSSION Pulmonary artery catheters in their course of passage to PA are fraught with coiling and knotting.[1],[2] A safe distance of 50 cm mark is recommended by various investigators.[3] In this patient after looking at the anatomical changes, it was apparent that the failure to reach right ventricle even after a significant catheter length (50 cm mark) was not due to coiling of PA catheter inside right atrium but in fact related to anomalous long venous path all along the posterior surface and the left border of the left ventricle and its opening into the inferior vena cava and the right atrium in this patient. In mitral stenosis patients with left atrial dilatation and pulmonary hypertension, we have reported that the PA catheter allocation into left pulmonary artery is significantly common and wedging takes place at shorter length of PA catheters.[4] However, in this patient, an unduly long length of catheter had to be inserted to enter the pulmonary artery. This caused concern and apprehension during the procedure. The diagnosis of anomalous venous connection and absent superior vena cava was missed during echocardiography, probably due to focus on the mitral valve disease. It could not be suspected during balloon mitral valvotomy as the balloon catheter was passed through the femoral vein and the inferior vena cava was draining normally into right atrium. Balloon valvoplasty was performed trans-septally entering into left atrium. Thus it failed to reveal the anomalous venous connection. Unaware of the anomalous venous connection, we faced considerable difficulty in placement of the pulmonary artery catheter. However, continuous cardiac output catheter could be placed by the usual method of tracking the waveform. In conclusion, we wish to emphasize that pulmonary artery catheter insertion may be problematic in patients with anomalous venous connection. During echocardiography in patients with dextrocardia, it is essential to look for other congenital anomalies. Although pulmonary artery waveform monitoring is a practical and successfully used guide for pulmonary artery catheter placement, in the presence of congenital cardiac abnormalities, additional guidance by fluoroscopy is advisable for the catheter placement. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04063f1.jpg] [ms04063f2.jpg] |
| |||||||||

{kind=link}
{kind=link}