 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 58, No. 10, October, 2004, pp. 417-422 Original Article Greek stroke score, Siriraj score and allen score in clinical diagnosis of intracerebral hemorrhage and infarct: Validation and comparison study Soman Aamod, Joshi ShashankR, Tarvade Sanjay, Jayaram S Department of Medicine, Grant Medical College & Sir
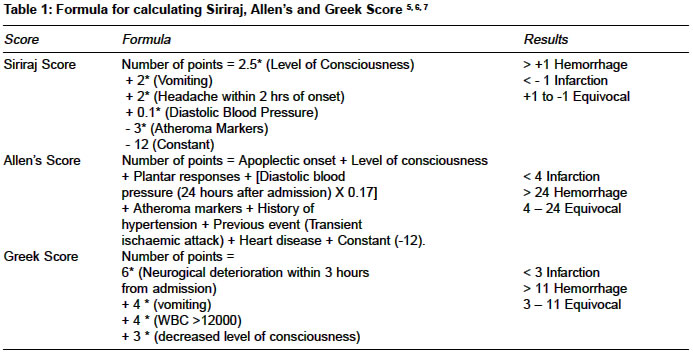
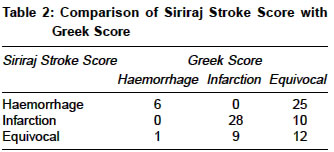
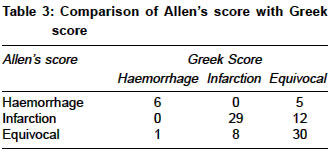
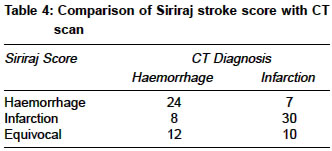
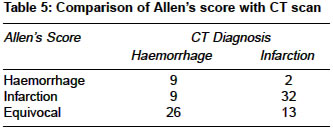
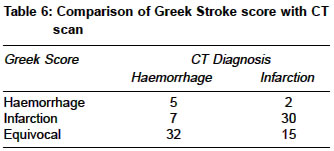
JJ Group of Hospitals, Mumbai - 400008 Code Number: ms04070 ABSTRACT AIM: To compare Greek stroke score with available previous two stroke scores for the diagnosis of cerebral ischemia and hemorrhage in acute stroke patients, and validate the Greek stroke score. KEY WORDS: Siriraj stroke score, Greek stroke score, Allen score, Comparison, validation. INTRODUCTION There are two famous stroke scores which can guide the treating physician in clinical distinction of hemorrhagic and ischemic stroke: Siriraj Scoring System and the Guys Hospital Scoring System, which have been studied at various centers in India for efficacy. Akpunonu et al studied the accuracy of Siriraj Stroke score and concluded that the sensitivity was 36% for the hemorrhagic stroke and 90% for the non hemorrhagic stroke, and the positive predictive values were 77% and 61% respectively.[1] Comparison of the two scores has been done in many studies. These studies have concluded that the Siriraj score is better than the Guy′s hospital score but at the same time the sensitivity of the Siriraj score has been in the range of 80 - 90%.[2],[3] However, a recently conducted study by Wadhwani Jyoti, et al showed that the sensitivity of Siriraj stroke score was 92.54% in diagnosing infarction and 87% for hemorrhage and its overall accuracy was 91.11%. The Guy′s hospital score had a sensitivity of 93.42% in diagnosing infarction, 66.66% for hemorrhage and overall accuracy of the score was 87%.[4] Recently, a new score proposed by a team from Athens claimed that the sensitivity, specificity, positive predictive value and negative predictive value were much better as compared to the previous scores.[5] This Greek Score has not been validated in India. Our aim was to compare new scoring system (Greek stroke score) with the Siriraj stroke score and Allen′s stroke score and validate the new stroke score in Indian settings. MATERIALS AND METHODS Ninety one patients of acute cerebrovascular accidents, admitted in a single Tertiary care Hospital in India were randomly enrolled in this study for duration of one year (Jan to Dec 2002). Inclusion criteria were: patients whose neurodeficit lasted for more than 24 hours and CT scan showed supratentorial cerebral infarction or intracerebral hemorrhage. Exclusion criteria used were: patients with stroke due to other causes like tuberculosis, tumors or trauma, patients who had insufficient data to calculate scores and patients with subarachnoid hemorrhage were excluded. Approval of Ethics committee of the hospital was sought prior to starting the study. Written informed consent was signed by patients before enrolling. Authors collected the data and stroke scores were calculated for each patient independently. The following patient variables were recorded: age, gender, history of previous stroke, TIA, IHD, Rheumatic heart disease, peripheral arterial disease, hypertension, diabetes, smoking, alcohol consumption, hyperlipidemia, clinical signs, and symptoms (onset of deficit, headache, vomiting, blood pressure, Glasgow Coma Scale, pupil and plantar response, neck stiffness, level of consciousness, neurological deterioration within the first 24 hours) and basic laboratory data (ECG, WBC count). Data was also utilized to study epidemiology of stroke. A form containing variables for all the three scores was filled by authors, and the definitions and guidelines were followed as per the original scores. CT scan was done in all the patients. The scores were calculated from the above variables (Formulas for calculation in [Table - 1])[5],[6],[7] and they were compared in ′certain′ results i.e. percentages of scores in which the scores predicted ischemia or hemorrhage according to the cutoffs suggested in the original papers. Results were considered to be certain when Allen score was <4 and >24, <-1 and >1 for Siriraj stroke score and Greek Score was <3 and >11. Kappa statistics were determined for agreement between two scores for certain cases. The results of three scores were compared with results of CT scan study. Sensitivity, specificity. Positive predictive value and negative predictive value were calculated for diagnosis of hemorrhage. We used Kappa statistics program for comparability test. RESULTS Out of 91 patients, 47 patients (51.64%) had cerebral infarction and 44 patients (48.35%) had intracerebral hemorrhage by Computed Tomography. Using Kappa statistics the overall comparability for certain cases of Greek Score with Siriraj stroke score was fair. (K=0.27) [Table - 2] and with Allen′s score was good (K=0.51) [Table - 3] The Siriraj Stroke score diagnosed 38 patients as cerebral infarction and 31 patients as Intracerebral Hemorrhage while 22 patients were in equivocal category. Thus the Score had a sensitivity of 0.75 (95% CI: 0.63, 0.84), specificity of 0.81 (95% CI: 0.71, 0.89), positive predictive value 0.77 (95% CI: 0.65, 0.86) and a negative predictive value of 0.78 (95% CI 0.69, 0.86) for diagnosis of Intracerebral Hemorrhage. [Table - 4] The Allen′s stroke score diagnosed 41 patients as cerebral infarction and 11 patients as Intracerebral Hemorrhage while 39 patients were in equivocal category. Thus the score had sensitivity of 0.50 (95% CI: 0.34, 0.58) specificity of 0.94 (95% CI: 0.86, 0.98), positive predictive value of 0.81 (95% CI: 0.56, 0.95), and negative predictive value of 0.78 (95% CI: 0.71, 0.81) for diagnosis of Intracerebral Hemorrhage. [Table - 5] The Greek Score diagnosed 37 patients as intracerebral hemorrhage, 7 patients as cerebral infarction and 47 patients were in equivocal category. Thus the Greek Score had a sensitivity of 0.416 (95% CI: 0.23, 0.53), specificity of 0.94 (95% CI: 0.87, 0.98), positive predictive value of 0.71 (95% CI: 0.39, 0.91) and a negative predictive value of 0.81 (95% CI: 0.75, 0.85) for diagnosis of Intracerebral Hemorrhage. [Table - 6] Equivocal cases were 51% for Greek Score, 24% for Siriraj Stroke score and 42% for Allen′s score. DISCUSSION Management of stroke largely depends on differentiation of hemorrhagic from ischemic stroke. Clinical stroke score can help in the differential diagnosis of stroke in areas with limited CT scan facilities. These scores are simple, screening diagnostic tools at the bedside, especially in rural hospitals. However, it has been found that the scoring systems are relatively inefficient in differentiating strokes. Recently Siriraj stroke score and Guy′s hospital score was tested by Badam et al in Indian settings and found that both score are not sufficiently accurate to identify infarct from hemorrhage.[8] Kochar et al studied both the scores in an Indian setting and found that Siriraj stroke score had specificity of 73% and Allens score had specificity of 91% in diagnosing hemorrhage.[9] Our study has also shown similar results. Our study showed that Siriraj Stroke score and Greek stroke score were not comparable in certain results whereas Allen′s score and Greek stroke score had fair comparability. Using these two scores (Allen′s score and Greek stroke score) together can increase the accuracy but Allen′s score can only be calculated at the end of 24 hours hence combined use is restricted. Even though Greek Score and Allen′s score have specificity of 94% for diagnosing hemorrhage, Greek score is better than Allen′s as it can be calculated immediately on admission. When physician wants to ascertain diagnosis of hemorrhage at admission, use of Greek score is advisable. Siriraj stroke score was relatively easy to calculate and it can be calculated on admission. Greek Score has utilized hematological investigation of WBC count for calculating score. This is the first validation study in India for Greek stroke score. Sensitivity, specificity, positive predictive value and negative predictive value calculated were inferior to original study from Greek. As our study had a small cohort further study is required with large sample of patients to validate this score in India. Systematic diagnostic approaches studied here can be used as guide to treating physicians where computed tomography facility is not available. Our study shows that these clinical scoring systems do not exhibit enough accuracy to be applied safely if the use of antithrombotic treatment is to be considered. And use of these clinical stroke scores can only be limited to clinically classify strokes for academic purpose where CT scan facility is not available. Though the Greek Score is better than the Siriraj Stroke score and Allen′s score in differential diagnosis of stroke, further improvement will have to be done in the future Stroke scores to increase their specificity. In view of low specificity of stroke scores and complications involved in inadvertent anticoagulant use in hemorrhagic stroke the use of these scoring systems in the presence of CT scan facilities is unadvisable. CONCLUSION Greek score and Allen′s score has similar specificity in diagnosing hemorrhage but the later can be calculated only at the end of 24 hours hence, the Greek score is better that Allen′s score. The CT scan remains as a gold standard in differential diagnosis of stroke and scoring systems are used as a guide in management only when resources are limited and CT scan facilities are not available. These scoring systems require further improvement to increase specificity. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04070t5.jpg] [ms04070t3.jpg] [ms04070t1.jpg] [ms04070t4.jpg] [ms04070t6.jpg] [ms04070t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}