 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 58, No. 10, October, 2004, pp. 423-430 Original Article A prospective, randomised, double-blind study of comparative efficacy of immediate versus daily cleaning of stethoscope using 66% ethyl alcohol Parmar RameshC, Valvi ChayyaC, Sira Poonam, Kamat JaishreeR The Department of Paediatrics, Seth G.S. Medical College & K.E.M. Hospital, Parel, Mumbai - 400 012 Correspondence Address:Department of Paediatric Cardiology, Madras Medical Mission Hospital, 4-A, J. J. Nagar, Mugappair (E), Chennai - 600 050, Tamilnadu ramehsparmar@yahoo.com Code Number: ms04071 ABSTRACT OBJECTIVE: Studies have demonstrated frequent contamination of stethoscope and usefulness of different disinfectants. Albeit, studies on the precise mode of cleaning and frequency of cleaning are lacking. This study was carried out to determine efficacy of 66% ethyl alcohol as disinfectant, rate of recontamination without cleaning and benefits of daily versus immediate cleaning. KEY WORDS: Cleaning practices, Stethoscope, Efficacy, 66% ethyl alcohol. INTRODUCTION Hospital acquired infections are frequently caused by microorganisms in the hospital environment and are a significant cause of morbidity and mortality. They also result in increased health care costs. About one third of all nosocomial infection are preventable.[1] For planning preventive actions, it is essential to identify the reservoirs of microorganisms that cause nosocomial infections. Hands of the hospital staff, medical equipment such as catheters, surgical instruments, implants, ventilators, endoscopes, thermometers, ultrasound probes, otoscopes, etc. may all serve as the reservoir for microorganisms.[2],[3],[4],[5],[6],[7],[8],[9],[10] The stethoscope; a universal tool of medical profession is often used on multiple patients. Except in services such as Intensive Care Units and Neonatal Special Care Units a single stethoscope is often used for all indoor as well as outdoor patients. A routine of disinfection of stethoscope is hardly ever undertaken.[11],[12] Previous studies have demonstrated frequent contamination of stethoscope and usefulness of different disinfectants.[11],[12],[13],[14],[15],[16] Precise studies on the exact mode and frequency of cleaning of stethoscope are lacking. This stimulated us to undertake this study to determine the frequency and type of contamination of stethoscopes used in various areas of the hospital, the efficacy of disinfectant (66% ethyl alcohol) wipes, the rate of recontamination of the diaphragm with routine use without cleaning and benefits of daily versus immediate cleaning. MATERIALS AND METHODS This prospective double-blind study was carried out over a period of one year, at a large tertiary hospital with bed strength of 1800 and catering to about 5905 outdoor patients and 1527 inpatients daily. One hundred stethoscopes used by the medical personnel in various areas of the hospital comprised the study material. An attempt was made to take a sample of representative areas of the hospital departments and to obtain the most random sample possible (Simple stratified randomisation). Following initial randomisation a clinical open study was carried out. Further randomisation was not opted for, as it would have jeopardised the effective sample size. Cultures from the surface of diaphragm of the stethoscopes were obtained using a sterile cotton-tipped swab moistened with sterile normal saline (0.9%). These swabs were inoculated on blood agar plates. To maintain a consistency in obtaining the Colony Forming Unit (CFU) per culture, for later comparison, the culture was obtained by swabbing half of the diaphragm each time and the plating was done on half of the culture plate. A code was assigned to each sample and Microbiologist was blinded to the subgroup from which the sample was collected. The first sample was collected without cleaning and was inoculated on one half of the blood agar plate. The whole diaphragm was then cleaned with a swab impregnated with disinfectant (66% ethyl alcohol) and allowed to dry. The other half of the diaphragm was then swabbed and inoculated on the second half of the same blood agar plate. The concerned doctor was advised to use the stethoscope in the usual way. A repeat culture of the same stethoscope was taken at the end of 5 days and plated on a second blood agar plate. A note of number of patients examined by the concerned doctor was made. The diaphragm was then cleaned using disinfectant swab at the end of each day for four days. At the end of the 5th day, culture was collected from the stethoscope and plated on the third plate. The number of patients examined was recorded. Thus, for every stethoscope used in the study four cultures were collected.
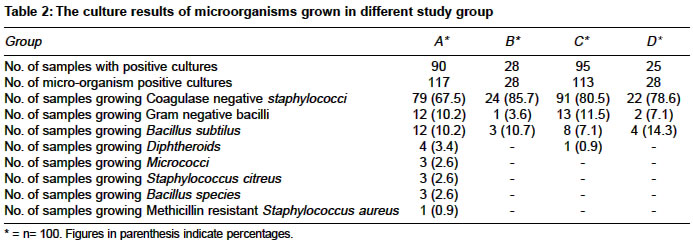
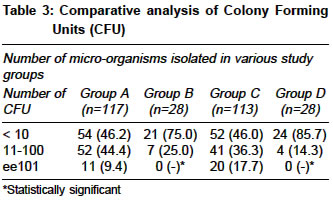
The results were decoded. The residual rate was calculated using the following formula for each subgroup. In addition, the medical staff was asked about the frequency of cleaning the stethoscope, the cleaning method used and if they received any instruction on cleaning of the stethoscope. Processing of the sample Antibiotic sensitivity was tested by the disk diffusion method as per the National Committee for Clinical Laboratory standards using 1 mgm discs. Statistical Analysis RESULTS The study sample of 100 stethoscopes comprised of those from paediatric wards (25), paediatric intensive care unit (15), medicine wards (40), and gynaecology and obstetrics wards (20) in each of the four study groups. Of the 100 doctors interviewed at the end of the study, none cleaned their stethoscopes regularly. Ten claimed to clean their stethoscopes intermittently when blood or human secretions soiled it and only two claimed that they cleaned their stethoscope once in a month or two. None had received any instruction on cleaning of the stethoscopes. In-group A, 90 of the 100 stethoscope (90%) were contaminated. 29 of these (22%) grew more than one microorganism. The service-wise break-up was as follows: 24 stethoscopes from the Paediatric Department (96%), 15 from the Paediatric Intensive Care Unit-PICU (100%), 33 from the Medicine Department (82%) and 18 from Gynaecology and Obstetric services (90%) yielded positive cultures. No statistically significant difference was found in rate of contamination of stethoscope among the different departments (P >0.05). The effect of cleaning of stethoscope with 66% ethyl alcohol is shown in [Table - 1]. Groups B and D both resulted in a significant reduction in the rate of contamination of the stethoscopes to 28% and 25% respectively. When the stethoscopes were used without cleaning (group C) the rate of contamination increased significantly (95%). No statistically significant difference was found between group A and C. A total of 117 and 113 positive microbial cultures were obtained from the 100 stethoscopes each in study Groups A and C respectively [Table - 2]; while in study groups B and D only 28 microorganisms were detected in each. The predominant organisms responsible for contamination were Gram-positive cocci. The predominant type of organisms isolated on the stethoscope was not dependent upon the department. The commonest microorganism from all the departments was CONS (70.4%, 70.6%, 68.2%, 62.0% of growth from stethoscope of paediatric, IPCU, medicine and gynaecology department respectively). No statistically significant interdepartmental variance was noted. Diphtheroids were isolated only from the stethoscopes used in the medicine department while micrococci were isolated only in stethoscopes used by gynaecologists. The comparative analysis of CFU in various study groups is shown in [Table - 3]. The total CFU in group A and C were 5165, and 9653, while group B and D it was 189 and 171 giving mean CFU count of 94.15, 6.75, 85.42, and 6.1 in groups A, B, C and D respectively. The mean residual rates were 5.2% and 3.65% in-groups B and D respectively. An attempt was made to correlate the degree of contamination with the number of patients examined by each stethoscope. In-group C the average number of patients examined per day was 30 and 28 for the culture positive and culture negative stethoscopes while in the group D, the corresponding figures were 27 and 25. These differences were not statistically significant. Antibiotic sensitivity revealed that 99.1% of CONS and all of GNB, Bacillus subtilus, diphtheroids, and micrococci were sensitive to Amoxycillin-Clavulinic acid. The sensitivity to cloxacillin was 68% for CONS, 3.5% for GNB 63% for Bacillus subtilus, 75% for diphtheroids, 67% for micrococci. DISCUSSION Most hospital-acquired infections are primarily nosocomial and not autoinfections.[17] Acquisition of infection in the hospital adds to the morbidity, mortality, and economic costs. Many, if not all, hospital-acquired infections result directly or indirectly from colonisation of the patients′ skin, gut or systems with hospital flora.[18] The colonised flora results in infection when the normal body defenses are impaired through underlying diseases, administration of immunomodulating therapy or use of invasive devices. Development of rational control methods for nosocomial infections thus, requires identification of reservoirs of pathogens that colonise the patients. Stethoscopes get contaminated by the organisms colonised on the patients′ skin, or those resident on the hands or outfits of the health care providers, or when they come in contact with blood and other biological secretions. The universal use of the stethoscope and its direct contact with multiple patients makes it an important potential factor in the dissemination of microorganisms from one patient to another. In hospitalised patients, this means an exposure of an already susceptible host to a higher microbial overload and for the patients attending Out Patient Department, an exposure to the ominous antibiotic-resistant hospital-flora. This is of particular relevance while treating renal transplant recipients, immunocompromised host, following cardiac surgery e. g. mitral valve replacement at the risk of serious infections. Studies have shown that only 0-3% of health care providers clean their stethoscopes regularly.[12],[13],[14] In our study, 10% cleaned it when blood or human secretions soiled it; and only two cleaned it at intervals of one to two months. This confirms the finding that hardly any stethoscope-cleaning practices exist among health care providers. Consistent with observation of others we found frequent contamination of stethoscopes. [10],[11],[12],[13],[14],[15],[16] In contrast to previous studies[13],[16] we did not find any interdepartmental variation. The commonest organism contaminating the stethoscope in the present study was CONS. Until recently infections due to CONS were regarded as endogenous in origin. However, there are now increasing reports on the endemic occurrence of distinct strains CONS. Several outbreaks due to CONS have been reported in neonates and patients undergoing cardiac surgery. GNB are important cause of nosocomial infection.[19],[20] Bacillus sp has been implicated in septicaemia.[21] Diphteroids are associated with nosocomial infections following invasive procedures as well as drug therapy.[22] MRSA amongst these are the most dreadful nosocomial pathogens associated with prolonged carriage and serious infections that are difficult to treat.[23],[24] We also isolated many potential pathogens such as Gram-negative bacilli, diphtheroids, bacillus sp., and MRSA. These findings conclude that isolation of CONS can no longer be considered innocuous and that potentially pathogenic organisms are carried on the stethoscope. It may be conceded that there are no studies linking the presence of micro-organisms on the stethoscope directly to hospital-acquired infection. However, strategies to reduce the occurrence of hospital-acquired infections should take this possibility into account. It is a well-known fact that disinfection or removal of contaminated equipment, like thermometer, has terminated outbreaks.[8] Therefore, cleaning or disinfecting the stethoscope can be considered important from the point of view of minimising the incidence of hospital-acquired infections. The next question refers to the choice of disinfectant and the schedule for its use. Stethoscopes were shown to harbour staphylococci as early as 1972. Yet standard sources on infection control give no advice about cleaning of stethoscope.[14] Wright et al and Breathnach et al demonstrated the utility of alcohol in disinfection, but no detailed studies were carried out in this regard.[12],[13] Jones et al reports isopropyl alcohol as the most effective disinfectant.[25] We chose ethyl alcohol as it is equally efficacious,[26] less expensive, readily available and rapidly bactericidal against vegetative organisms, and is tuberculocidal, virucidal and fungicidal, as well.[26] Its activity is probably related to its ability to denature proteins. It is suitable for disinfection of horizontal surfaces as it evaporates rapidly and tends to leave the equipment dry. Ours is the first study to show a systematic use of cleaning method using 66% ethyl alcohol. Its use resulted in a fall in the rate of contamination of stethoscopes from 90% (Group A) to 28% and 25% in group B (immediate cleaning) and group D (once daily cleaning), respectively. With a mean residual rate of 5.25% and 6.35% in-groups B and D respectively, it resulted in complete elimination of pathogenic microorganisms like MRSA, diphtheroids, micrococci, and Bacillus species, with drastic reduction in contamination by GNB and CONS. Even in these CFU count had dropped down significantly. This is important as not only the presence of microorganisms but also its actual load is important in occurrence of infection. The rate of contamination increased to 95% when stethoscopes were used without cleaning (group C). Considering the published literature and the efficacy demonstrated in our study, ethyl alcohol seems to be an effective and inexpensive agent for disinfection of the stethoscopes. The only disadvantage is its inflammability, which entails that it be stored with care. Ideal disinfecting agent for the decontamination of stethoscope should be one that is efficacious, readily available, and one that can be used without cost restraints and is non-cumbersome to use. 66% ethyl alcohol serves this important task and can be used in all the hospital both in developed world and developing countries. Studies have shown that stethoscope-cleaning practices are not only sub-optimal but that the health care personnel are stubbornly resistant to change these practices.[13] While advising a schedule, we have to ensure that there is reasonable decrease in the carriage of organisms on the stethoscope diaphragms. At the same time the schedule should be such that the health care providers will adhere to it. Although cleaning of stethoscopes after every use will be considered the most ideal manner of disinfecting it, it is tedious and time consuming. A study by Wright et al demonstrates this vividly.[13] They gave the responsibility of cleaning the stethoscopes to the health care personnel who were advised to do so 8 hourly. But even, these were not adhered to.[13] Hence, we decided to compare cleaning the stethoscopes on a daily basis versus after immediately after use and found that daily cleaning gives results that are equivalent to those obtained immediately on cleaning. Occasional cleaning, (group C) had no benefit at all. Therefore, if one has to decrease carriage of microorganisms on the stethoscopes, the health care personnel may be advised to clean it at least once a day. Although, the aspect of compliance was not studied in the project, it is reasonable to expect that the personnel will be able to subscribe to this not so demanding schedule. Another limitation of our study includes lack of fungal and viral cultures that could not be undertaken for financial constraints. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04071t3.jpg] [ms04071t2.jpg] [ms04071t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}