 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
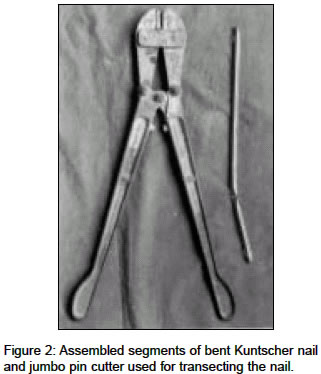
Indian Journal of Medical Sciences, Vol. 58, No. 10, October, 2004, pp. 439-441 Case Report An innovative technique to cut and extract loose bent Kuntscher nail Singh Roop, Sharma AshwiniK, Kiranpreet Department of Orthopaedics, Paraplegia, Rehabilitation, Postgraduate Institute of Medical Sciences, Rohtak - 124001 Code Number: ms04073 ABSTRACT Removal of a grossly deformed nail can be a serious and perplexing problem. We report an innovative technique to cut and extract a loose bent Kuntscher nail. The technique is simple and effective; can be used in peripheral hospitals where advanced gadgetries may not be present.KEY WORDS: Kuntscher nail, Transection, Extraction INTRODUCTION Intramedullary nailing has been a widely accepted method of treatment of fixation of fractures of femoral shaft. Bending and breaking of the nail are the most important complications specific to the concept. These complications are more prevalent if the fracture is unstable, goes to nonunion, implant is smaller in size or patient has refracture.[1] Removal of a grossly deformed intramedullary nail can be a serious and perplexing problem. We were recently faced with the problem of removing a loose and bent (about 35°) ten millimeters stainless steel Kuntscher nail in a 45-year old male with nonunion lower third of femur [Figure - 1].The Kuntscher nailing was done 6 months back in a peripheral hospital and was referred to our tertiary center for further management after having a fall. Manipulation under anaesthesia, to straighten the nail in-situ failed as the nail used to rotate inside the medullary cavity with external force. Relevant literature was scanned. Hacksaw with blades and a steel drill were arranged to transect/weaken the nail, but following innovative approach was used. TECHNIQUE There was a butterfly fragment at the nonunion site and bone grafting was contemplated in the case, we took advantage of both the factors. The nonunion site was exposed with a 7.5-centimetre, long skin incision, the butterfly fragment with its soft tissue attachments was tilted with the help of a Kocher′s forceps to expose the underlying nail. As the nail was of smaller diameter, an attempt was made to straighten it with a small punch and hammer before venturing into a more cumbersome method of transecting or controlled weakening of nail with drill. Instead of getting straight, nail got crumpled and we were able to cut with the help of a jumbo-pin cutter [Figure - 2]. Both parts of the nail were removed through the non-union site, as they were lying loose in both fragments. Biological osteosynthesis was achieved with a 12 hole AO/ASIF 95° condylar plate after giving two separate small incisions, under image intensifier control. Bone grafting was done at nonunion site. DISCUSSION An intramedullary nail imparts stability for a limited period of time until bone healing is attained. Complications like bending and fatigue failure of implant add to the woes of nonunions, delayed unions or refractures. Standard accepted method of treatment of a bent nail is to straighten it in-situ; remove it from proximal end; and go for exchange nailing.[2] Opening the fracture site and transecting[3],[4] or controlled weakening of the nail before removal[5],[6],[7] are the options available, if one is not able to straighten the nail in-situ through application of a substantial external force. Procedures like transecting or drilling the nail produce metal debris and there are chances of shattering of discs/burrs, drill bits or hacksaws. Soft tissues may be contaminated with metal debris and thermal necrosis of soft tissues and bone can occur due to heat generation while transecting or drilling. In the present case, it is hypothesized that nonunion caused the nail to fail. Six months duration is sufficient for a femoral diaphyseal fracture to heal .In the given circumstances, instead of unlocked intramedullary nail surgeon should have opted for locked intramedullary nailing or other suitable methods of osteosynthesis. We removed both the fragments of nail through nonunion site, as they were lying loose in both proximal and distal ends of bone. No extensive dissection or periosteal stripping was required due to presence of butterfly fragment. Otherwise; we recommend standard method of removing Kuntscher nail through proximal end after straightening or transecting it. Our method is simple and effective, as it does not produce metal debris and heat while cutting, allowing extraction of the bent nail. It may be useful even in high strength nails to produce sufficient weakening to straighten by manual manipulation; in the event one is not able to transect the nail completely. The procedure has also its application in peripheral hospitals, where advanced gadgetries for transecting the nail may not be present. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04073f2.jpg] [ms04073f1.jpg] |
| |||||||||

{kind=link}
{kind=link}