 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 58, No. 11, November, 2004, pp. 465-471 Original Article Association of serum antioxidants and risk of coronary heart disease in South Indian population Rajasekhar D, Srinivasa Rao PVLN, Latheef SAA, Saibaba KSS, Subramanyam G Departments of Cardiology, Sri VenkateswaraInstitute
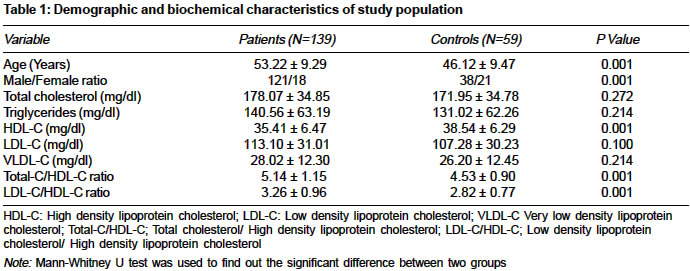
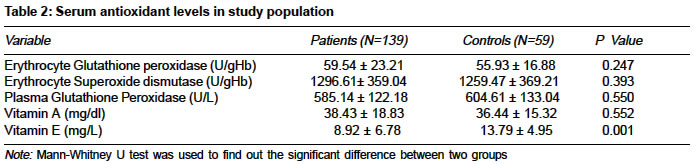
of Medical Sciences, Tirupati - 517507, Andhra Pradesh Code Number: ms04077 ABSTRACT BACKGROUND AND AIM: Higher prevalence of coronary heart disease (CHD) has been reported in south Indian population, which cannot be accounted for by the traditional risk factors like hyperlipidemia. Identification of new risk factors may help in treatment and prevention of CHD in this part of the world. In an attempt to investigate the causes of increased incidence of CHD in this part of the world, we intended to look for oxidative stress in our patients as a possible risk factor. As an initial step in this perspective, a case- control study was conducted to find out the serum antioxidant levels and their association with CHD in south Indian population. KEY WORDS: Coronary heart disease, Lipids, Lipoproteins, Antioxidants, South India. INTRODUCTION Coronary heart disease (CHD) is a leading cause of morbidity and mortality in developed countries and is emerging as an epidemic in developing countries.[1] It is predicted that there will be an increase of 111% in cardiovascular deaths in India by the year 2020 when compared to the year 1990.[2] This is much higher than that predicted to any other region both in Asia as well as outside Asia. In India, the prevalence of CHD is much higher in south when compared to north India.[3],[4] This high prevalence warrants probing into the presence of various risk factors and their association with CHD. Traditional risk factors like serum cholesterol, blood pressure and smoking account for not more than 50% difference in mortality of CHD.[5] This led to studies on newer risk factors like fibrinogen, Lp(a), plasminogen activator, antioxidants etc. Harman first suggested oxidation of biopolymers as etiology in aging.[6] Oxidative modification hypothesis of atherosclerosis originated with the observation of Goldstein et al.[7] Oxidized LDL has been identified in atherosclerotic lesions.[8] This has prompted the study of antioxidants in the prevention of the initiation and progression of cardiovascular disease.[9] Descriptive, case-control and prospective cohort studies have found inverse associations between the frequency of coronary heart disease and dietary intake of antioxidant vitamins.[10] Case-control studies[11],[12],[13] have shown low levels of serum antioxidants in CHD patients when compared to controls and suggested the role of Vitamin E in prevention of CHD. In India Dube et al[14] (Jaipur), Nand et al[15] (Haryana) and Singh et al[16] (Moradabad) have reported deficiency of serum vitamin E levels in CHD patients. In one study efficacy of antioxidant vitamins was tested on serum lipid profile and lipid peroxide levels in a clinical trial which lasted for 30 days. Decreased lipid peroxide levels were observed in supplemented group as compared to placebo group.[17] But the results of the prospective studies have been equivocal. As a result some considered this as a set back for antioxidant therapy as well as oxidative hypothesis of atherosclerosis. However, a closer examination of these reports reveal many lacunae like improper design of trial, inadequate dosage of antioxidant vitamins, improper selection of patients.[18],[19] Hence, we studied the serum antioxidant levels and their relation to coronary heart disease in south Indian population as there are no reports from this part of world. MATERIALS AND METHODS One hundred thirty nine consecutive patients attending cardiology clinic from November, 2000 to November, 2002 and willing to get enrolled in the study formed the patient group. Coronary heart disease status was confirmed by angiographic evidence. The patient group included 79 smokers, 66 diabetics and 51 hypertensives. Fifty patients had a family history of CHD. Age of the patients ranged from 29-75 years. Patients with pancreatic insufficiency, cystic fibrosis, betalipoproteinemia or small intestinal resection were excluded. Fifty nine population-based controls free of clinical CHD (substantiated by 12 lead rest ECG and history) were included in the study. Their age ranged from 29-72 years. An ethics committee of our Institute cleared the protocol for execution of the study. Informed consent of the subjects was taken for participation in the study. Fasting blood samples were drawn from subjects who were on 12 hour fasting. Triglycerides, total cholesterol (total-C) and high density lipoprotein cholesterol (HDL-C) were estimated using commercial kits on the synchron cx4 analyzer from Beckman Instruments Inc., California, USA. Erythrocyte and plasma glutathione peroxidase and superoxide dismutase activities were measured using Ransel and Ransod kits (Randox Laboratories Limited Crumlin, UK) on the same analyzer. Low density cholesterol (LDL-C) and very low density lipoprotein cholesterol (VLDL-C) were calculated using Friedewald′s formula.[20] Total-C/HDL-C and LDL-C/HDL-C ratios were calculated. Serum Vitamin A and E were measured simultaneously by high performance liquid chromatography.[21] Hemoglobin was estimated by the cyanomethemoglobin method using commercial kits. Statistical Analysis RESULTS Mean ± S.D values of demographic, lipid and lipoprotein parameters factors are presented in [Table - 1]; serum antioxidant levels in patients and controls are shown in [Table - 2]. Total-C/HDL-C and LDL-C/HDL-C ratio (P<0.001) were significantly higher and HDL-C (P<0.002) levels were lower in patients when compared to controls. Significantly lower levels of vitamin E in patients than in controls (P<0.001) were observed. No significant difference of serum and erythrocyte glutathione peroxidase activity and superoxide dismutase activity and serum levels of vitamin A were observed between patients and controls. The association of vitamin E with CHD remained inversely significant even after controlling for age and other coronary risk factors (sex, smoking, diabetes, family history, total cholesterol, triglycerides, HDL cholesterol and VLDL cholesterol). DISCUSSION An important implication of oxidative modification hypothesis of atherosclerosis is that antioxidants may inhibit atherogenesis, through mechanisms like protection of LDL against oxidative modification. Antioxidant enzymes are present in small amounts only in plasma and other external fluids. Besides these, antioxidants like Vitamin E are of major importance. Increased prevalence of coronary heart disease necessitated the intervention that can reduce the risk of CHD. Hence, correspondingly greater attention is being focused on prevention of CHD. In this area antioxidants may serve an important role. Activity of glutathione peroxidase was shown to be increased in blood and decreased in erythrocyte, whereas decreased or no change in super oxide dismutase was reported in patients than in controls in earlier studies.[22],[23],[24] Our study did not reveal any change in the antioxidant enzymes of blood in patients with CHD when compared to the control group. Also, administration of antioxidant enzymes to improve the antioxidant defense has its own practical implications. Hence the attention logically gets diverted towards the antioxidant vitamins. Decrease or no change in concentration of vitamin A was observed in earlier studies.[16],[25] In the present study also no significant changes in vitamin A levels were observed in patients when compared to controls. However, there was a significant decrease in the plasma vitamin E levels in patients with CHD when compared to healthy controls (P<0.001). This is in agreement with other reports.[11],[14],[15],[16] Vitamin E is a lipid soluble peroxyl radical scavenger in human cells. Vitamin E interrupts lipid peroxidation by scavenging peroxyl radical intermediates. Vitamin E may inhibit cell mediated LDL oxidation by reducing cellular production and release of reactive oxygen species. Beneficial effects of vitamin E includes inhibition of smooth muscle cell proliferation, preservation of endothelial function, inhibition of monocyte-endothelial adhesion, inhibition of monocyte reactive oxygen species and cytokine release, inhibition of platelet adhesion and aggregation, protection of LDL against oxidation, increased resistance of LDL to oxidation as well as, lowering of cytotoxicity of oxidized LDL towards endothelial cells.[10],[25],[26],[27] Because of this multiple beneficial action, emphasis with respect to the study of antioxidant status as well as its improvement revolves round vitamin E. Also the ease of administration and lack of side effects add to the concept. Patients with pancreatic insufficiency, cystic fibrosis, betalipoproteinemia or small intestinal resection are at increased risk of vitamin E deficiency.[28] Our study did not include any patient with above mentioned disorders. Decreased serum vitamin E levels may be due to the reduced intake or smoking.[29] Reduced levels of vitamin E may also be due to the increased requirement of vitamin E in pro-oxidant milieu with enhanced free radical status, leading to the increased lipid peroxidation, a resultant depletion of free radical scavenger and antioxidant reserves of the body.[30] Esterbauer et al[31] have reported that endogenous antioxidants, mainly tocopherol, contained in LDL particles are rapidly consumed after induced oxidation and propagation of the oxidative process doesn′t begin until antioxidant molecules are largely exhausted. Low levels of vitamin E was associated with increased risk of CHD.[26] Significant inverse association of vitamin E and CHD was observed in studies conducted in India and abroad.[12],[16] In our study also we have observed significant inverse relation of serum vitamin E with CHD after adjustment for age, sex, smoking, diabetes, hypertension, family history of CHD, lipids and lipoproteins (Odds ratio 0.898, 95 CI% 0.826-0.976 P<0.01). Diabetes, hypertension and smoking, which are known to produce oxidative stress are present in the patients studied and might have contributed to the low levels of vitamin E observed in our study. However, the significant association observed between vitamin E levels and CHD even after correcting for these factors points towards a greater attention to this and treat this as an independent risk factor. Further efforts are on to identify the local causes of low vitamin E levels and the effects of vitamin supplementation on the CHD incidence. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04077t2.jpg] [ms04077t1.jpg] |
| |||||||||

{kind=link}
{kind=link}