 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
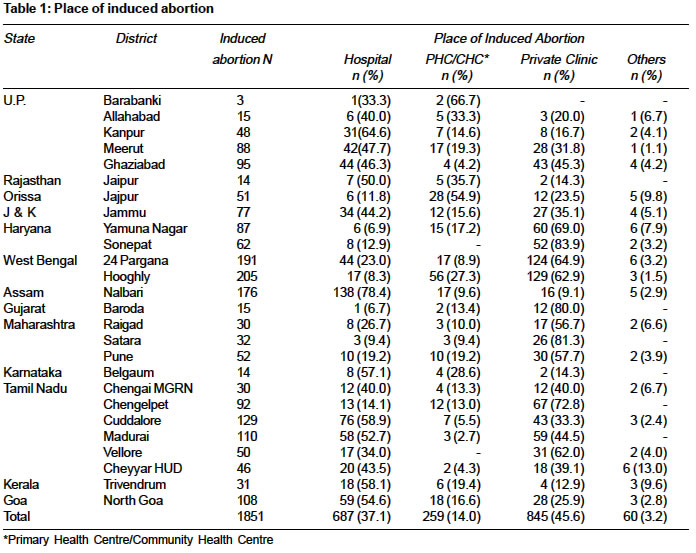
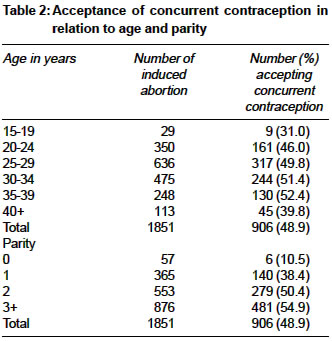
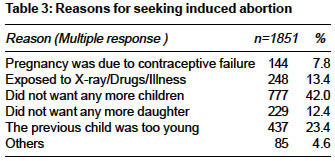
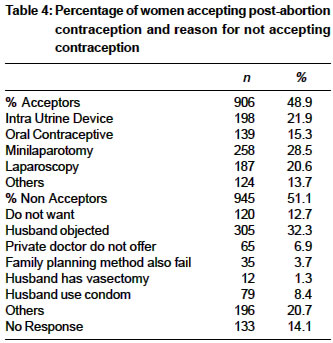
Indian Journal of Medical Sciences, Vol. 58, No. 11, November, 2004, pp. 478-484 Original Article Induced abortion and concurrent adoption of contraception in the rural areas of India (An ICMR task force study) Dhillon BS, Chandhiok N, Kambo I, Saxena NC Division of Reproductive Health and Nutrition, Indian Council of Medical Research, Ansari Nagar, New Delhi - 110 029 Code Number: ms04079 ABSTRACT BACKGROUND: Despite a liberal Medical Termination of Pregnancy (MTP) act and awareness of family planning, maternal mortality attributable to induced abortion is high.AIMS: Assess attitude, behavior, practices and utilization of services by rural women for induced abortion and concurrent acceptance of contraception. SETTINGS AND DESIGN: Cross sectional survey of eligible married women in 13 states in India over one year. MATERIAL AND METHODS: A total of 1851 women who had an induced abortion during the previous 3 years were interviewed. STATISTICAL ANALYSIS USED: Includes proportions, rates and chi-square test. RESULTS: The main reason for seeking abortion was "don't need any more children" (42%), and in 12.4 per cent they specifically mentioned that they "don't need any more daughters". Around 46% of women accessed abortion services from private clinics as compared to government hospital (37.1%) and Primary Health Centre/Community Health Centre (14.0%). The decision to terminate the pregnancy and place of abortion was made by the husband in 42.8% and 52.5% respectively. Regret for abortion was expressed by 29.6% of the women. However, only 7.2% said they would not advice others for induced abortion. Nearly one half of the women undergoing abortion accepted a family planning method concurrently; of these Intra Uterine Device/oral contraceptives and a permanent method was adopted by 37.2% and 49.1% respectively. Acceptance of vasectomy by male partner was found to be low (1.3%). "Husband objected" (32.3%) was the main reason for not accepting post abortal contraception. Majority of the acceptors said they would recommend to others the same place where they had undergone abortion, thus indicating their satisfaction with the source and services received. CONCLUSIONS: Counselling for post-abortal contraceptive should be provided to the couple so that they can make an informed choice. KEY WORDS: Induced, abortion, contraception, rural, India. INTRODUCTION Safe and legal abortion is considered a key intervention for improving women′s health and quality of life. Despite a liberal abortion law in India, (Medical Termination of Pregnancy Act of India 1971)[1] of 6.7 million induced abortions every year[2] only 10 percent are conducted under safe conditions.[3] Most of the abortions, especially in the rural areas, are conducted illegally by untrained personal under unhygienic and unsafe condition. These lead to a high maternal morbidity and mortality and contributes to about 9 to 12 percent of maternal deaths.[4],[5] Even where the services are available they are underutilized. This is mainly due to lack of knowledge among the community regarding the legality and availability of abortion services, cultural sensitivity, un-compassionate attitude of the provider, hesitancy to avail services from male provider and lack of post abortion care.[6] Although there are indications of a steady increase in the number of abortions over the years,[6] data on attitude, behavior and practices related to abortion are not very conclusive. This information is necessary for improving the accessibility and utilization of abortion services and increasing the concurrent adoption of contraception. The Indian Council of Medical Research (ICMR) initiated a project on Integrated Reproductive Health Care Delivery through its network of Human Reproduction Research Centres (HRRCs) located at medical colleges in various regions of the country. The present paper is based on observations related to induced abortion, studied during the course of a large reproductive health survey of eligible married women conducted in the rural areas of various parts of India. MATERIALS AND METHODS A multi indicator cluster survey of eligible women (married, aged 15-45 years), covering various reproductive health issues including induced abortion, was conducted in 26 districts from 13 states of the country between January 1996 to February 1997. A three stage stratified random cluster sampling was adopted for selection of villages from the rural areas for the survey. Selection of districts was done by the HRRCs in consultation with the district health authorities. Stratification for sampling of villages was done at two stages on the basis of distance from the health facilities. In the first stage, blocks were stratified into two groups based on distance from the District Hospital and one block was selected randomly from each group. In the second stage, villages in the two selected blocks were stratified into three groups on the basis of distance from Primary Health Centre (PHC), presence of subcentre (SC) in the village and remote village thus forming six strata. At the third stage, random clusters (villages) were selected from each stratum to provide coverage of about 4000 eligible women from the district. Questionnaires for the survey were prepared centrally in English and were translated into regional languages at the respective HRRCs. The questions pertaining to women′s perceptions, opinions, knowledge, attitudes etc. were open-ended and the probable responses were listed to facilitate recording and minimizing interview time. No leading or suggestive questions were asked to avoid courteous responses and over estimation. Women were interviewed at their homes by female interviewers. Only volunteered responses were recorded. Necessary instruction manuals were prepared and regional workshop of HRRC medical officers were held for discussing conduction of the survey. Selection of the interviewers was done locally by the HRRCs. Training of interviewers was carried out by the HRRC medical officers. A total of 1851 women who had an induced abortions during last three years were identified from a survey of 1,17,465 eligible married rural women and interviewed in detail about the reason for seeking abortion, utilization of services and post abortal contraceptive practices. Data analysis was carried out at the ICMR Headquarters. Statistical analysis includes simple percentage distribution, rates and c2-test. RESULTS The number of cases reported varied from 3 in Barabanki district of Uttar Pradesh to about 200 from the Hooghly district of West Bengal. More than hundred cases of induced abortions were reported from the districts of 24 Parganas and Hooghly, West Bengal; Nalbari, Assam; Cuddalore and Madurai, Tamil Nadu; and North Goa, Goa [Table - 1]. The mean age of women who underwent abortion was 29.2 ± 5.7 years. Three-fifths of the induced abortion seekers were between 25-34 years and in 47.3 per cent the parity was three or more. A small percent of induced abortion were in adolescent (1.6%) and in nulliparous women (3.1%) [Table - 2]. The most common reason given for terminating the pregnancy was "did not want any more children" (42%). Other reasons included "child too young" (23.4%), "exposure to X-ray/illness" (13.4%), "pregnancy due to contraceptive failure" (7.8%), and "others" (4.6%). In 12.4 per cent women the reason for abortion was specifically mentioned "do not want any more daughters". However, information on whether abortion in these women was conducted after pre-natal sex-determination was not elicited [Table - 3]. Almost 85 per cent of women said that the decision to terminate the pregnancy was made by the husband (42.8%) or self (42.2%). The role of mother-in-law, health functionaries and others in facilitating the decision was mentioned by 5.7, 5.4 and 3.9 per cent of women respectively. The selection of health facility for induced abortion was made by the husband in 52.5%, herself in 14.5%, and mother-in-law in 6.2% of cases. Suggestions in this respect made by health functionaries and others including relatives/friends/neighbors, to the women seeking abortion were 14.4 and 12.4 per cent respectively. The most common place for abortion was reported to be the "private clinic" (45.6%). Other places included "hospital" in 37.1%, "Primary Health Centre/Community Health Centre" (PHC/CHC) in 14.0%, and "other" in 3.3%. More women had gone to private facility than to hospital, CHC or PHC from the study districts of Haryana, West Bengal, Gujarat, Maharashtra and Madurai and Vellore districts from Tamil Nadu [Table - 1]. Post-abortion contraception was accepted by 48.9 per cent of the women. Of these, 37.2 per cent accepted an Intra Uterine Device/oral contraceptive (IUD/OC) and 49.1 per cent a permanent method. In addition, husbands of 11 women (1.3%) had accepted vasectomy. [Table - 4] As expected, acceptance of concurrent contraception showed significant positive association with increasing age (c25 =11.2, P=0.047) and parity (c23=63.02, P<0.001) [Table - 2]. The main reason given for not accepting any post-abortion contraceptive was "husband objected" (32.3%). Other reasons included "do not want" (12.7%), "private doctors do not offer" (6.9%), "Family Planning method fails" (3.7%). In 8.4 per cent, the women mentioned that husband was using condoms while 20.7% did not respond [Table - 4]. There were 29.6 per cent women who mentioned that they regret having gone going through an induced abortion. In more than half of these women (57.5%) the decision to terminate the pregnancy was taken by the husband and in a quarter by the woman herself (25.8%). However, on asking women whether they recommend others for induced abortion services, only 7.2 per cent replied that they would not advice an induced abortion. As compared to Hospital and Private clinic, fewer women got the desired services at PHC or CHC (c23= 496.4, P<0.001). There were 371 women who had initially gone to PHC for induced abortion, but only 140 (37.7%) could get the desired services. Of these 107 (76.4%) women said that they would recommend PHC for abortion services. Of the women who had gone to Hospital, CHC or private clinic, 89.7, 82.0, and 68.7 per cent respectively said they would recommend the same place to others desiring induced abortion indicating that as compared to private clinic, women were more satisfied with services obtained from government health facilities like PHC, CHC and hospitals. (c23= 64.4, P<0.001). DISCUSSION Worldwide the magnitude of abortion represents an important aspect of women′s reproductive health and rights. Even though there is a marked increase in the number of legal abortion acceptors since the enactment of the MTP act in India, illegal abortion is still three (urban) to five (rural) times more common than legal abortion.[7] The increase in legal abortion acceptors may be due to awareness about MTP act, changing attitude of women towards abortion, improvement in the availability of hospital facilities and declining social stigma attached to abortion. However, it is difficult to say how far there is a real increase in the number of MTP acceptors as some of them may otherwise have undergone illegal abortion. The present study has brought out that a very large proportion of women (45.6%) had availed abortion services from private clinic in comparison to government hospital or PHC/CHC. Although India has more than 1 billion people, records from 1996 indicate that there were only 8511 approved institutions where abortions could be performed legally.[3] Abortion services also vary tremendously by region. For instance, Maharashtra State has 23 recognized institutions per million populations, whereas India′s most populous state, Uttar Pradesh, has only 4 approved centers per million.[3] Moreover, even in Maharashtra only 76 (5%) of 1646 approved centers are functioning. ICMR national survey on quality of services (1991) revealed that out of 200 block PHCs, 91 PHCs (45.5%) were registered for MTP but only 25 per cent had adequate equipment to conduct abortion. Further, in only 88 PHCs, there was a trained doctor for conducting MTP.[8] In a study carried out in Gujarat, it was observed that out of 53 registered PHCs visited, only 15 (28%) were actually providing the services. In the rest, either due to unavailability of equipment or trained manpower, services were not being provided.[9] Most women also prefer sources that are not public (like PHC or CHC) and go to private clinics where privacy and confidentiality are better maintained. Another motivating factor for seeking abortion services from private clinics is because they do not insist that a woman should adopt a concurrent contraceptive method. In our series, majority of the acceptors said they would recommend to others the same place where they had undergone abortion, thus indicating their satisfaction with the source and services received. Many women consider abortion as a method of contraception. This is supported by the fact that in our study the reason for abortion given in 42 percent was that they did not want any more children and in only 7.8 percent it was due to failure of contraception. Of concern, is that post-abortion contraception was only accepted by 48.9 per cent of the women. Though awareness of contraception is high,[10] lack of availability of spacing methods, misinformation and apprehension about the different contraceptive options prevents widespread contraceptive use and abortion is used as an alternative to contraception. It was observed in a study that although post abortion clients clearly wanted to avoid another unwanted pregnancy, they generally failed to receive family planning information and services. Abortion providers did not view contraceptive provision as their responsibility and, in many cases, had negative attitudes toward abortion patients. Services for abortion and family planning often were not available on the same day or in the same location. In some areas in India, contraceptive provision was coerced as a condition for abortion.[11] In rural areas particularly husbands′ approval is strongly associated with abortion and contraception use among women. In the present study, in majority of cases, the "decision to terminate the pregnancy" (42.8%) and "place of abortion" (52.5%) was decided by the husband. In addition, in one-third of the cases, "husband objected" was the reason given for non-acceptance of post abortion contraception. By providing counselling to the couple it is expected that acceptance of post abortion contraception will improve. The role of health functionaries in facilitating the decision or selection of health health facility was low. About 30 per cent of the women expressed their regret for undergoing the procedure, though the decision for MTP was largely taken by themselves and their husbands. Considering the large number of women expressing regrets after accepting MTP, it is important to undertake an in-depth study to understand the causes of such regrets and circumstances under which decision was taken for abortion. CONCLUSION The study indicates that there is need to strengthen MTP services at PHC/CHC level to meet the demand in rural areas and train the health care providers in pre and post abortion care. Non-surgical methods and manual vacuum aspiration technique of abortion should be introduced at PHC level to increase the accessibility and utilization of abortion services. The health care provider should not insist for post abortion contraception but provide information and counseling to enable the women and spouse to make an informed and voluntary choice and thus avoid the need of a repeat abortion. Contraceptive services should also include emergency contraceptives to prevent unwanted pregnancy due to unprotected sex. Advocacy for safe abortion services needs to be made after ensuring adequate facilities in rural areas. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04079t4.jpg] [ms04079t3.jpg] [ms04079t2.jpg] [ms04079t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}