 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 58, No. 12, December, 2004, pp. 513-519 Original Article Prevalence of Aspergillus species in clinical samples isolated in an Indian tertiary care hospital Xess Immaculata, Mohanty Srujana, Jain Neena, Banerjee Uma Department of Microbiology,All India Institute of
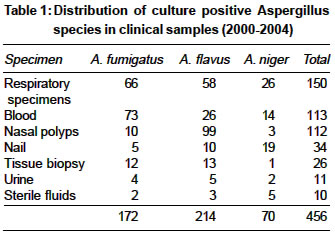
Medical Sciences, New Delhi - 29 Code Number: ms04084 ABSTRACT CONTEXT (BACKGROUND): In recent times, it has become important to determine the prevalence of different Aspergillus species in clinical samples in view of difference in antifungal susceptibility noted in some species.AIMS: To determine the species prevalence of Aspergillus isolates in various clinical samples received in the Mycology Laboratory at our institute. METHOD: Over a period of 4-years, a total of 18,731 samples were processed, and species identification carried out by standard microbiological methods. RESULTS: Four hundred and fifty six samples (2.43%) were culture positive for Aspergillus species. A.flavus (46.93%) was the most common isolate, followed by A.fumigatus (37.72%) and A.niger (15.35%). It was observed that A.fumigatus was the predominant species isolated from blood and respiratory specimens, A.flavus was predominantly isolated from nasal polyps whereas A.niger predominated in nail specimens. Culture positivity was highest in the age group 12-65 years and in males. Sixty-nine patients (15.13%) were admitted to the intensive care unit. CONCLUSIONS: The study highlights the diverse manifestations caused by Aspergillus species in human beings and also throws light on the different species prevalent locally. The knowledge would prove useful in selecting empirical antifungal therapy and formulating prophylactic and pre-emptive strategies. KEY WORDS: Aspergillus species, clinical samples, fungemia. INTRODUCTION Aspergillus species are saprophytic, thermotolerant fungi that are ubiquitous in the air and the environment.[1] Though humans inhale Aspergillus spores at the rate of hundreds per day, they rarely experience complications.[2] However, under special circumstances, Aspergillus species can produce a spectrum of diseases, including allergic bronchopulmonary aspergillosis, aspergilloma, chronic necrotizing aspergillosis, and life-threatening invasive aspergillosis.[3],[4] In addition, endocarditis, paranasal sinus granuloma, keratitis, otomycosis and onychomycoses caused by Aspergillus species have also been described in the literature.[1],[3] Since its first description as an opportunistic infection in 1953,[5] there has been a substantial increase in the number of cases of invasive aspergillosis documented at autopsy in all developed nations. One major teaching hospital in Frankfurt, Germany, showed a 14-fold increase in the number of cases over the years 1978-1992.[6] A national autopsy survey conducted in Japan from 1970 to 1995 showed that the incidence of invasive aspergillosis increased from 0.4% to 1.4% during that period.[7] Despite the substantial worldwide clinical use of antifungal agents, invasive aspergillosis continues to remain the most common invasive mold infection worldwide.[1] Though approximately 900 species have been described till date, remarkably only a few species cause disease and equally remarkably, those same species cause multiple diseases.[3] The most common ones causing invasive disease include A.fumigatus, A.flavus, A.niger, A.terreus and A.nidulans.[1] A.fumigatus accounts for ~ 90% of cases of invasive aspergillosis though an increasing number of cases of aspergillosis due to species other than A.fumigatus is now being reported.[8] The increase in the number of cases of aspergillosis may perhaps be attributed to the fact that in recent times, there has been a substantial increase in the number of patients at risk of developing invasive aspergillosis including the advent of AIDS, the development of new intensive chemotherapy regimens for solid tumors, lymphomas and leukemias, increase in the number of bone marrow and solid organ transplant recipients and increased use of immunosuppressive regimens for other autoimmune diseases.[9],[10],[11],[12] As other supportive care is improved and most bacterial infections successfully treated, the importance of invasive aspergillosis has increased over time. Until recently, it has not been therapeutically important to determine which species of Aspergillus is causing disease because no differences in outcome have been noted between infections caused by different species. Recently, however, some differences in susceptibility to itraconazole, other azoles and amphotericin B have been noted between species.[13],[14] Furthermore, an emerging fungal pathogen, Aspergillus terreus, has often been found to be refractory to amphotericin B.[15] Thus, clinically significant Aspergillus isolates need to be identified to the species level. Keeping the above facts in consideration, we did the present retrospective analysis to study the species prevalence of Aspergillus isolates in various clinical samples at our institute. MATERIALS AND METHODS Aspergillus isolates All strains of Aspergillus species isolated from clinical samples received in the clinical Mycology Laboratory, Department of Microbiology at the All India Institute of Medical Sciences, New Delhi over a 4 - year period from April 2000 to March 2004 were included in the study. They were isolated from blood cultures in cases of blood stream infections (n=113), respiratory tract specimens in cases of pulmonary aspergillosis (n=150), nasal polyps in cases of paranasal sinus mycoses (n=112), nail in cases of onychomycosis (n=34), tissue (n=26), urine (n=11) and sterile fluids (n=10). Sample processing and identification of isolates Sample processing and identification of isolates was done according to standard mycological techniques.[16] All samples (except blood) were inoculated on two sets of Sabouraud′s Dextrose Agar medium containing gentamicin (0.065 %). These were incubated at 25°C and 37°C and examined daily for a period of four weeks before declared as culture negative. Blood samples were cultured on a biphasic medium (Sabouraud′s Dextrose Agar and broth) and incubated at 37°C for a period of at least four weeks before declaring culture negative. Direct 10% potassium hydroxide and Gram′s stain preparation was also done on all samples except blood. Culture positive specimens were identified as Aspergillus species both macroscopically and microscopically by observing the colony characteristics and by a lactophenol cotton blue mount preparation respectively. An effort was made to confirm every positive culture by processing repeated and consecutive samples and demonstrating precipitins in serum by Ouchterlony′s agarose gel double diffusion technique[17] using a commercially available antigen (Meridian Diagnostics, USA). However, depending on the availability of serum samples from patients, the gel diffusion technique could be performed only on 93 specimens. RESULTS Out of a total of 18,731 samples processed over a period of 4-years in our laboratory, 456 samples (2.43%) belonging to 430 patients were culture positive for Aspergillus species. The highest number of isolates belonged to A.flavus (46.93%) followed by A.fumigatus (37.72%). Aspergillus niger accounted for the least number of isolates (15.35%) [Table - 1]. A.fumigatus was the predominant isolate from blood and respiratory specimens, A.flavus was predominant in nasal polyps from cases of paranasal sinus mycosis and A. niger was the commonest isolate from specimens of nail. From tissue samples, both A. fumigatus and A. flavus were isolated in almost equal proportions. As regards demographic characteristics, maximum culture positivity was observed in the age group 12-65 years (80.0%) and in males (68.2%). The number of culture positive samples in the age group 0-12 years was 62 out of 456 (13.6%) and in elderly patients above > 65 years was 29 out of 456 (6.35%). Sixty-nine patients (15.13%) were admitted to the intensive care unit. Amongst the 113 blood samples which grew Aspergillus species, 39 belonged to patients with hematological malignancies (36 leukemia, 1 Ewing′s sarcoma, 1 multiple myeloma and 1 aplastic anaemia), 51 samples were obtained from patients who were immunocompromised in varying degrees depending upon the cause (36 with long term antibiotic intake, 6 HIV positive patients, 4 with long term steroid intake, 3 patients with diabetes and 2 transplant recipients), 5 samples were from patients with rheumatic heart disease and 18 were obtained from patients with pyrexia of unknown origin. Multiple blood samples with the same Aspergillus species were positive in 6 patients (2 cultures positive in 4 patients and 3 cultures positive in 2 patients). Of the 112 nasal polyps, 64 were from maxillary sinus, 11 from ethmoid sinus, 5 from sphenoid sinus, 4 from frontal sinus and site of 28 specimens was not known. Of the 34 samples with onychomycosis, 7 were obtained from nails of hands and 15 from nails of toes; site of 12 nail samples was not known. The distribution of the 26 tissue specimens as per site was as follows: 3 were vegetations from heart valves in cases of rheumatic heart disease, 2 were from orbital bones, 2 ear tissues, 1 ocular, 1 lung, 1 nasal crust, 1 skin tissue whereas site of 15 samples was not known. Of the 10 sterile fluid specimens, 3 consisted of cerebrospinal fluid, 2 were blister fluids, 2 were pleural fluid specimens, 2 peritoneal fluid and 1 bile. Of 150 respiratory tract specimens, 72 were obtained from patients characterized as allergic bronchopulmonary aspergillosis, 10 were from cases of aspergillosis (characterized as such based on history, clinical signs/ symptoms and radiological findings), 35 were obtained from patients suspected of fungal pneumonias (of these 30 had haematological malignancies, 3 had cystic fibrosis and 2 were HIV positive), 26 samples were obtained from patients with chronic obstructive pulmonary disease (19 chronic asthmatics, 7 bronchiectasis patients) and 7 specimens were obtained from miscellaneous patients. In total, the number of patients having samples repeatedly culture positive with the same species of Aspergillus were 26 (6 blood samples and 20 samples from other sites). Out of the 93 serum specimens subjected to the gel diffusion technique, 6 were positive (6.45%). DISCUSSION The incidence of invasive aspergilius in different studies varies from < 1% to 40% depending on the patient population.[18] The incidence of aspergillosis observed in our institute (2.43%) is thus similar to that seen in others. However, contrary to previously published reports where A.fumigatus has been responsible for approximately 90% of infections, the present study demonstrates A.flavus to be the predominant isolate. Allergic bronchopulmonary aspergillosis (ABPA) is a complex condition that results from hypersensitivity to the fungus.[3] First described in the United Kingdom in 1952, it has been estimated to occur in 1-2% of chronic asthmatics[19] and up to 13.6% of patients with cystic fibrosis.[20] In our study too, we isolated the fungus from patients with cystic fibrosis and chronic asthma. In bronchopulmonary aspergillosis and aspergilloma, inhalation is the most important method initiating infection from soil, rotting vegetables, leaf piles, dung heaps etc.[3] In the present study there was preponderance of aspergillosis in males and younger persons which leads to the possible explanation that males spend more time outdoors and in fields and thus acquire the agent from the locally prevalent fungal flora. A large proportion of A.flavus isolates (99 out of 214, 46.26%) were from patients with paranasal sinus mycoses, where it has been observed to be the most frequent causative agent in earlier studies.[21],[22],[23] Furthermore, maxillary and ethmoid sinuses were the commonest ones to be involved as observed previously.[21] Criteria for differentiating true Aspergillus fungemia from contamination have been proposed by Duthie and Denning.[24] Definite aspergillus fungemia was defined as the growth of Aspergillus species from blood cultures associated with either histological evidence of hyphae in tissue from other sites or positive cultures for the same Aspergillus species in the setting of a clinical condition compatible with invasive aspergillosis (i.e. pulmonary infiltrate and Aspergillus isolation from sputum cultures).[24] Only one of our patient could be categorized as definite Aspergillus fungemia. Probable aspergillus fungemia was defined as the growth of Aspergillus species from blood cultures in a patient with clinical signs of aspergillosis, but without mycobiological or histopathological evidence of invasive aspergillosis (i.e. pulmonary infiltrate requiring amphotericin B therapy).[24] The rest of the patients in the present study fall into this category. As mentioned above, most of these patients were immunocompromised in varying degrees or had underlying malignancies or bone marrow disorders. Thus, this study suggests that the incidence and severity of Aspergillus infection can be reduced by early identification of high risk patients establishing fungal etiological agent and targeted for antifungal therapy. As regards nail infections, we observed an isolation rate of 7.9% (36 out of 456) which is in accordance with those from others where the fungi has been isolated from 2%[25] - 10.36%[26] of cases of onychomycosis. Some studies though have found a low isolation rate of Aspergillus species from nail infections (1 out of 111 positive cultures).[27] Similar to other studies,[26],[28] we also found A.niger to be the commonest nail isolate. Other Aspergillus species recovered from nail infections include A.nidulans [26] and A.terreus.[27] Aspergillus spp have also rarely been isolated from unusual sites[1] like CSF, pericardium, peritoneum, vascular grafts, bones etc which we have also observed. In summary, the present study highlights the diverse manifestations caused by Aspergillus spp in human beings. Human aspergillosis is generally seen in chronic debilitating conditions such as lympho and myeloproliferative diseases, AIDS and HIV positive individuals, leukemia, transplant recipients etc, who are on immunosuppressant therapy. Since ours is a tertiary care hospital with an increasingly large number of patient population with such underlying disorders, it is logical to expect an increase in the occurrence of invasive aspergillosis in near future. Furthermore, they continue to remain the most common causes of invasive mold infections in immunocompromised patients. Thus, there is a need to develop a greater understanding of the pathogenesis of the disease, formulate better and more sensitive diagnostic techniques, develop superior antifungal agents and increase an awareness of the disease among clinicians. More important is the need to develop antifungal susceptibility testing for Aspergillus species and means to prevent occurrence of the disease specially in immunocompromised individuals. A knowledge of local patterns of infection and antifungal susceptibility would prove useful in selecting empirical therapy and formulating prophylactic and pre-emptive strategies. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04084t1.jpg] |
| |||||||||

{kind=link}