 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
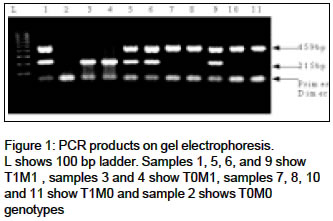
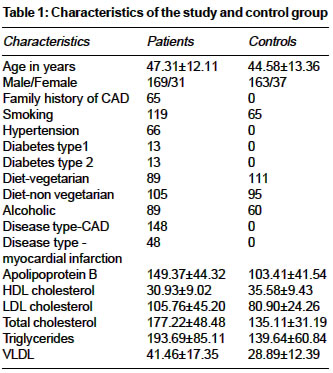
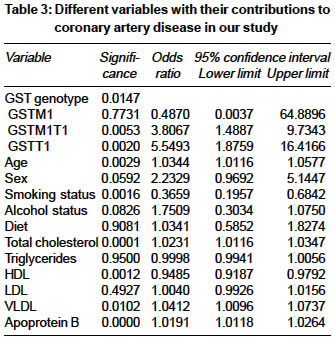
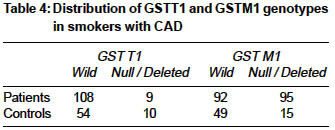
Indian Journal of Medical Sciences, Vol. 58, No. 12, December, 2004, pp. 520-526 Original Article T1 and M1 polymorphism in glutathione S-transferase gene and coronary artery disease in North Indian population Girisha KM, Gilmour A, Mastana S, Singh VP, Sinha N, Tewari S, Ramesh V, Sankar VH, Agrawal Suraksha Departments of Medical Genetics, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow - 226014 Code Number: ms04085 ABSTRACT BACKGROUND: DNA damage has been found to play an important role in atherosclerosis and coronary artery disease. Genetic polymorphisms of the genes coding for enzymes involved in the metabolism of genotoxins result in different phenotypes with respect to their ability to detoxify these agents. In the present study the contribution of the polymorphism in the glutathione S-transferase gene to the development of coronary artery disease has been investigated.METHODS: One hundred and ninety seven angiographically proven patients with coronary artery disease and one hundred and ninety eight age-matched controls were genotyped for glutathione S- transferase polymorphism by polymerase chain reaction. Genotype frequencies were compared in patients and controls by Chi-square test. Binary logistic regression was used to examine the relationship between genotype and disease, incorporating other variables into the model. RESULTS: GSTT1 null genotype was significantly decreased in patients with coronary artery disease. No significant association was found with GSTM1 genotypes. No such association was seen with smokers. CONCLUSION: Null genotype of GSTT1 is protective against coronary artery disease in our population. Key Words: Glutathione S-transferase, Smoking, Coronary Artery Disease, Polymorphism. INTRODUCTION The potential role of DNA damage in atherosclerosis has been a subject of research. DNA damage, as evidenced by DNA adducts and oxidative DNA damage has been observed in vascular tissues. Higher levels of DNA adducts in vascular tissues than in other tissues have been reported.[1],[2],[3] Polycyclic aromatic hydrocarbons, which are genotoxic, are shown to promote atherosclerotic plaque development.[2] It has been observed that DNA adduct levels are higher in patients with severe coronary artery disease than in patients with lower degree of stenosis.[4] Heart disease mortality rates correlated with levels of oxidative DNA adducts in peripheral blood lymphocytes in a study carried out in five European countries and these DNA adducts have been found to be at a higher level in atherosclerotic plaques suggesting their role in pathogenesis[1],[4],[5] In experimental animals, chemicals in tobacco smoke have been reported to induce and stimulate atherosclerotic plaque formation.[2],[6] Glutathione S-transferase (GST) forms a multigene family of phase II detoxification of polycyclic aromatic hydrocarbons. This plays an important role in protecting DNA against damage by genotoxins and adducts formation.[7] The polymorphism in the GSTT1 and GSTM1 gene loci is caused by a gene deletion. This results in virtual absence of enzyme activity in individuals with the GSTT1 and GSTM1 null genotypes. This has been confirmed by phenotype assays that have demonstrated 94% or greater concordance between genotype and phenotype.[8],[9] The polymorphisms affecting the activity of this enzyme may affect the processes contributing to the development of atherosclerosis. The association of polymorphisms in the glutathione S-transferase (GST) gene with coronary artery disease and myocardial infarction has been the subject of many investigations.[10],[11],[12] In the present study we have tested the hypothesis that the loss of activity of the enzyme due to a deletion polymorphism in the GSTT1 and GSTM1 may affect the risk of developing CAD. PATIENTS AND METHODS The patients with coronary artery disease in the study were evaluated at the department of cardiology of Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow. Our institute is a tertiary referral center with population draining from northern Indian states. Diagnosis of CAD was based on the presence of >50% stenosis in one of the coronary arteries. An experienced cardiologist who was blind to the study performed angiography. Age matched controls were selected after a detailed evaluation of history, clinical features, including a treadmill test to exclude the presence of CAD. Controls were healthy volunteers (hospital staff and attendants of patients with unrelated conditions) and did not have any of the risk following factors: history of ischaemic heart disease in the family, diabetes mellitus and hypertension. Informed consent was obtained from all subjects and the ethics committee of the institute approved the study. Polymorphism in glutathione S-transferase (GST) gene DNA was extracted by salting out method. T1 and M1 polymorphism on the GST gene was studied by amplification of the genomic DNA using the following primers: GST T1 forward primer: 5′- TT CCT TAC TGG TCC TCA CAT CTC - 3′ The primers were synthesized by Invitrogen Life Technologies, UK. The final concentration used was: 0.5mM of each primer, 1.5 units of Thermoprime Plus DNA polymerase, 75mm Tris-HCl (pH 8.8 at 25° C), 20 mM ammonium sulfate, 2.5 mM MgCl2, 0.01% Tween 20, 0.02 mM each of dNTPs and 0.5 mL of template DNA (100 ng/mL) per reaction. Annealing temperature was 58° C. After 35 cycles the PCR product was visualized with 2% agarose gel electrophoresis at 125V for 45 minutes. The GSTT1 product was 459bp and GSTM1 product was 209bp in size. Internal controls were used to check the amplification in cases with null genotypes Genotyping Allele frequencies were calculated by gene counting methods. Presence of the particular allele was designated as wild genotype and homozygous absence or deletion of the allele was designated as null genotype [Figure - 1]. Statistical analysis Genotype frequencies in various groups were compared by Chi-square test. Binary logistic regression was used to examine the relationship between genotype and disease, incorporating other variables into the model. All analyses were performed using SPSS v9.00 (SPSS Inc.) statistical analysis software. RESULTS Out of 200 individuals each in study and control group, the final data on polymorphism was obtained only on 197 patients and 198 controls. The characteristics of the study and control groups are shown in [Table - 1]. It is evident from the table that the distribution of age between patient and controls was not significantly different. The mean ages ± SD of patient and controls were 47.31 ± 12.11 and 44.58 ± 13.36 years respectively. Glutathione S-Transferase (GST) T1M1 polymorphism The distribution of GST genotype in the study subjects is shown in [Table - 2]. The genotype frequencies were in Hardy-Weinberg Equilibrium. Our results revealed a significantly lower frequency of GSTT1 null genotype in patients with coronary artery disease (P=0.0029) as compared to the control group. GSTM1 genotype frequency was similar in both the study groups (P=0.6084). The incidence of CAD in those with wild GSTT1 was 52.9% and in those with null genotype was 29.4% (with odds ratio of 2.70 at 95% confidence interval of 1.424-5.106) Logistic regression was used to examine the relationship between the genotype and the disease with the occurrence of disease as dependent variable with binary outcome [Table - 3]. Other variables were incorporated into the model as independent variables. It is seen from the table that GST genotype influences the occurrence of CAD. This model predicted the occurrence of the disease with 81.22% accuracy. Among the other variables, significant association was found with age, smoking status, cholesterol, HDL, VLDL and apoprotein B levels. Sex, alcoholism and diet did not reveal any significant association The genotype distribution was analyzed with respect to the smoking status. 182 nonsmokers and 162 smokers had GSTT1 wild genotype and 32 nonsmokers and 19 smokers had GSTT1 null genotypes. Wild GSTM1 was found in 167 and 141 nonsmokers and smokers respectively whereas null GSTM1 genotype was found in 47 and 40 nonsmokers and smokers respectively. There was no significant difference of genotype frequency in smokers and nonsmokers. The genotypes in smokers were analyzed with respect to the disease status [Table - 4], no significant association between genotype and occurrence of coronary artery disease in smokers was seen. However we found an association of coronary disease with GSTT1 wild genotype in nonsmokers (P-0.018, OR-2.969, 95% confidence interval 1.165-7.570). DISCUSSION The present study was conducted to look into the relationship between the genetic polymorphism of glutathione S-transferase, which is involved in the metabolism of genotoxins like polycyclic aromatic hydrocarbons. There are very few studies on the association of GST polymorphism with CAD in the literature; more interestingly, no report from India has been published. Wilson et al have published two similar studies, one in migrant South Asians and the other in Caucasians.[10],[11] In South Asians, they have found that the GSTM1 null phenotype was associated with lesser incidence of CAD (P=0.029 OR=0.63), but no significant association was observed between the GSTT1 wild genotype and CAD (P>0.05).[10] Results were similar in their earlier studies on Caucasians.[11] Our findings are not in concordance with Wilson et al as we have observed the GSTT1 genotype association with CAD in North Indian population but not with GSTM1 variant. However, Wilson et al have reported that the individuals carrying GSTM1 null genotype have a low risk of CAD. The OR was higher in this study as compared to their studies (2.7 v/s 0.63). It is possible that the difference in the populations is because of differences in geographical origins of South Asian samples. In our study both control and cases were from a well characterized population. Moreover, the sum total of the activity of isoenzymes may determine the metabolic effect rather than individual enzymes. As tobacco smoking is known to induce DNA damage, the relationship of polymorphism of enzymes involved in the metabolism of genotoxins with development of CAD has been looked into specifically by Wilson et al and Tamer el al.[11],[13] Wilson et al have reported a significant association with smoking status and hypothesized that the tobacco smoking induced DNA damage is the underlying mechanism in causing the CAD. Tobacco smoking has been shown to cause DNA damage and induce formation of DNA adducts. In a recent study Tamer et al found a significant GSTT1 null genotype association with smoking status and heart disease in Turkish population.[13] They found that the null GSTM1 and GSTT1 genotypes were associated with an increased risk of developing coronary heart disease but this increase was not significant. However, they found smokers, with null genotypes of GSTT1 and GSTM1 were at a significantly higher risk of coronary artery disease. There are various reports on association of GST polymorphisms with cancers.[14],[15],[16] Based on these evidences we have also analyzed the genotypes in smokers separately. We have seen that the association of CAD was not significant with GST polymorphism in smokers. The significance of association of GSTT1 did not increase in smokers as compared to the entire study population. It is possible that the decreased activity of GST affects the various mechanisms of DNA damage, including those mediated by tobacco and oxidative stress. However, in South Asians Wilson et al have also not found any relationship with smoking.[10] These results demonstrate that GST polymorphism may act differently in different ethnic groups. However, these conflicting results implicating different genotypes as a risk factor for CAD suggests a need for further work in this direction. It is difficult to determine the role of polymorphism of different proteins involved in the inflammation in CAD. The studies of this kind have limitations in establishing the causal role in the disease. However, these studies contribute to the scientific evidence in elucidating the etiology of complex multifactorial diseases like CAD and hopefully provide a step in the search for candidate genes. ACKNOWLEDGEMENTS Authors acknowledge the financial support provided by Uttar Pradesh Center for Science and Technology (UPCST) and Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04085t1.jpg] [ms04085t4.jpg] [ms04085t3.jpg] [ms04085t2.jpg] [ms04085f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}