 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
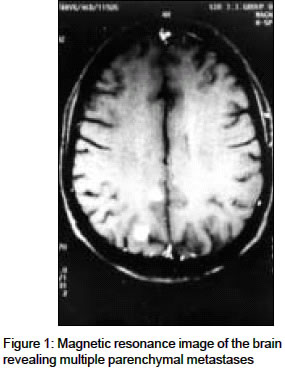
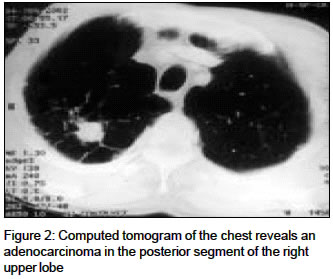
Indian Journal of Medical Sciences, Vol. 58, No. 12, December, 2004, pp. 530-532 Letter To Editor Meningeal carcinomatosis - An unusual cause of multiple cranial nerve palsies and sensory neuropathy Shenoy VV, Tarvade SM, Nagar VS, Deshpande AK Department of Medicine, Grant Medical College & Sir J. J. Group of [Govt.] Hospitals, Mumbai Code Number: ms04088 Sir, Neurological manifestations of a distant primary malignancy can occur due to intraparenchymal metastasis, leptomeningeal carcinomatosis and paraneoplastic syndromes.[1] Leptomeningeal carcinomatosis is diffuse involvement of meninges by the tumor cells and involves the cerebral hemispheres, cranial nerves & spinal cord and roots.[2] We present a patient with rare combination of all the three forms of extensive neurological involvement due to dissemination from a silent primary site. A 60-year-old man presented with progressive weakness in right upper and lower limbs, impaired hearing in right ear, and diminished vision in right eye over past one month. Later he developed inability to close right eye and deviation of angle of mouth to left side. There was no headache, fever, convulsions, or altered sensorium. On neurological examination, visual acuity was diminished in the right eye, but well preserved in the left eye (6/18). A sensorineural deafness and lower motor neuron facial palsy on the right side were noted. There was hypotonia on right side with normal power on both sides. He had decreased pain, joint position and vibration sense on right side. All reflexes were diminished and plantars were extensor on right side. CT scan of brain was normal. CSF examination showed 70 cells with 60% lymphocytes with normal sugar and proteins. Pure tone audiometry revealed bilateral sensorineural deafness, more severe on the right side. Electrophysiological studies revealed generalized sensory neuropathy. MRI with gadolinium contrast revealed multiple intraparenchymal lesions with enhancement [Figure - 1] in both cerebral hemispheres. A repeat CSF cytology detected adenocarcinoma cells and confirmed the diagnosis of Meningeal carcinomatosis. CT scan of chest revealed a solitary pulmonary nodule [Figure - 2] in the posterior segment of right upper lobe. Transpleural CT guided biopsy of the lesion confirmed an adenocarcinoma. The patient was discharged after 5 cycles of radiotherapy and was lost to follow up. First described by Eberth in 1870, meningeal carcinomatosis has an incidence of 1-5% in all solid tumors and is a presenting manifestation in 6-38% of unknown primary malignancy,[2] commonly adenocarcinomas of lungs, breast, gastrointestinal tract, melanomas[3] and rarely ovarian malignancy.[4] Deafness due to meningeal carcinomatosis was first described by Saenger in 1900; since then less than 20 cases have been published.[2] Although headache and mental status changes are common presentations, multiple cranial nerve palsy is also a known feature. The most commonly involved cranial nerves are occulomotor, abducens and trigeminal nerves in solid tumors and the facial nerve in leukemic meningitis.[3],[5] CT scans are normal in about 60% of the cases while gadolinium enhanced MRI has a sensitivity of about 70%.[5] MRI may demonstrate thickening of nerve roots, subependymal or pachymeningeal enhancement, or multiple enhancing nodular deposits. The gold standard for diagnosis is CSF cytology; though positive in only 60% cases, its sensitivity increases to 85% after 3 lumbar punctures. Lymphocytic pleocytosis as in this case is strongly supportive. This case had a rare presentation with involvement of unusual cranial nerves (II, VII, & VIII), intraparenchymal metastasis, and paraneoplastic sensory neuronopathy. The treatment of meningeal carcinomatosis consists of radiotherapy (2400rads) with chemotherapy using methotrexate, cyto-A, and thio-tepa. The prognosis is usually gloomy, median survival being 4-6 weeks after diagnosis. Though meningeal carcinomatosis is uncommon, this case emphasizes the need for detailed neuroradiological and oncological investigations with repeated CSF in patients with progressive cranial nerve palsies of apparently unknown cause. REFERENCES
Copyright 2004 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms04088f2.jpg] [ms04088f1.jpg] |
| |||||||||

{kind=link}
{kind=link}