 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 59, No. 1, January, 2005, pp. 13-19 Original Article Medical equipment in government health facilities: Missed opportunities Pardeshi GeetaS Department of Preventive and Social Medicine, R.C.S.M.,
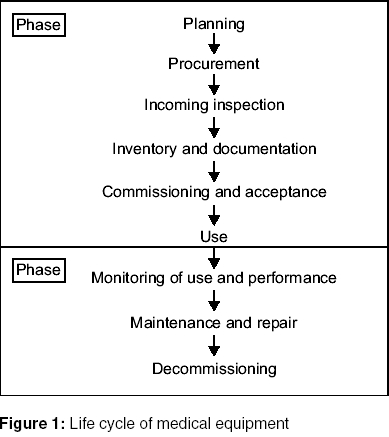
G.M.C, Kolhapur Code Number: ms05003 ABSTRACT BACKGROUND: The availability and optimal utilization of medical equipment is important for improving the quality of health services. Significant investments are made for the purchase, maintenance and repair of medical equipment. Inadequate management of these equipment will result in financial losses and deprive the public of the intended benefits. This analysis is based on the conceptual framework drawn from the WHO recommended- lifecycle of medical equipment.AIMS: (1) To identify the problems in different stages of the life cycle. (2) To assess its financial implications and effect on service delivery. SETTINGS AND DESIGN: Analysis of secondary data from the latest Comptroller and Auditor General (CAG) Reports for the states in India. The study variables were category of equipment, financial implications and problems in the stages of life cycle. STATISTICAL ANALYSIS: Calculation of proportions. RESULTS AND CONCLUSIONS: A total of forty instances mentioning problems in the first phase of the life cycle of medical equipment were noted in 12 state reports. The equipment from the radiology department (15), equipment in the wards (5), laboratory (3) and operation theatres (4) were the ones most frequently implicated. In a majority of cases the financial implications amounted to twenty-five lakhs. The financial implications were in the form of extra expenditure, unfruitful expenditure or locking of funds. In 25 cases the equipment could not be put to use because of non-availability of trained staff and inadequate infrastructural support. Careful procurement, incoming inspection, successful installation and synchronization of qualified trained staff and infrastructural support will ensure timely onset of use of the equipment. KEY WORDS: Medical Equipment, lifecycle, utilization INTRODUCTION Equipment is an integral part of the physical infrastructure of a health setup. It is an important means of providing various diagnostic and therapeutic services to the people. The availability and optimal utilization of the medical equipment contributes to the improvement of the quality of health services. The additional collateral benefits achieved are it avoids unnecessary referrals, provides an opportunity to learn and train the students in the medical colleges and makes research possible.The purchase, maintenance and repair of the medical equipment amounts to a large investment of funds. The role of the sophisticated technical equipment for diagnosis and management of diseases is also rising by the day. In addition, the various external-aided programs and health system development projects have also resulted in the purchase of sophisticated equipment in large numbers. A few studies have pointed out the sub-optimal availability and utilization of equipment in the government health centers and hospitals. The ICMR survey of 1991 has reported that the availability of essential instruments was not adequate in many subcentres and the PHCs (Primary Health Centers).[1] The RCH facility survey in 1999 noted that in India, 89% of the district hospitals, 49% of the CHCs (Community Health Centers) and 56% of the PHCs have at least 60% of the required medical equipment with regional variations.[2] Conceptual framework The World health Organization has described the life cycle of the medical equipment.[3] The life cycle approach has been recommenced for a comprehensive and more effective management of the medical equipment. It is important to manage each stage in the lifecycle for better results. The conceptual framework for this study is based on this life cycle approach. The life cycle of the medical equipment is divided into two phases. Phase I: Till the equipment is put into use. Each of these stages is further divided into different stages [Figure - 1]. This study assesses some of the problems in the different stages of Phase I in this lifecycle. MATERIALS AND METHODS The latest Comptroller and Auditor General of India (CAG) reports available for the states in India by July 2004 were reviewed carefully. The reports mentioning problems in the different stages of Phase I of the life cycle were included in the study. The instances leading to sub-optimal utilization of medical equipment were studied and analyzed. The variables considered were type of equipment, financial implications and reasons for sub-optimal utilization. The statistical analysis was done using proportions. The Comptroller and Auditor General of India examines various aspects of government expenditure in different sectors and undertakings. These aspects include: Audit provision of funds, Audit against rules and regulations, Audit of sanctions to expenditure, Propriety audit and efficiency cum performance audit. Audit boards are constituted for conducting comprehensive audits. These boards associate with them experts in the relevant disciplines, discuss their findings with the institutional authorities, controlling ministries and respective departments to ascertain their findings. The results of such comprehensive appraisals are incorporated by the CAG in his reports. RESULTS A total of 27 reports were reviewed. Of these, one was a report for the year 1999,seven were for the year 2001 and 19 were reports for the year 2002. Out of these, twelve (44%) reports mentioned medical equipment A total 40 instances describing problems in one or more stages of the life cycle of the medical equipment were noted. The category of equipment according to the department/section in which it is used is given in [Table - 1]. A majority of the equipment is from the radiology department, which includes diagnostic imaging equipment like X-rays, CT Scan, USG and Cardiovascular sector scanner. In one report 15 PHCs were reported to have idle X-ray machines. The equipment in the wards included Mobile C-arm imaging system, ventilator, Blood Gas Analyzer (ICCU), fetal monitor (NICU) and equipment for emergency wards. The Laboratory equipment were Refrigerated blood bank centrifuge, Auto-analyzer and Trinoculor research microscope. The equipment in the operation theatre not in use were cautry, Bypass surgery equipment, angiography machine and OT light. Problems were noted with the cobalt therapy units in the radiotherapy department. The supportive equipment included steam sterilizers, incinerator and steam laundries. The orthopedic implants, imaging films, subcentre instruments and ophthalmic equipment were included in the others category. In four instances only mention of hospital equipment was made without further specification. In 21 cases the equipment was purchased for Medical colleges, seven for public hospitals, eleven for PHCs and one was for subcentre. The main problems identified in the early part of the life cycle were in purchase, non-availability of trained staff and problems during installation. [Table - 2] During purchase the problems encountered were: (a) Delay in arranging necessary certificates, delay in civil works, late receipt of funds for building thereby leading to delay in supply. Problems were also noted in other phases of the life cycle. [Table - 2] In one instance defective X-Ray unit was purchased because of improper incoming inspection. In one case there was no centralized store inventory. Direct allotment was made to different departments. This resulted into non-projection of the year-wise procurement, issues and balances lying unutilized in the store. A shortage of Imaging films in the MRI/CT Scan unit worth 8.06 lakhs indicated the possibility of pilferage of scanning facilities in the hospital. In another case the equipment purchased for the emergency wards were distributed to other wards. Even after the purchase of the equipment like radiotherapy units, CT Scans, X-ray machines could not be installed for want of space, rooms or three phase electric connections. In 15 cases the equipment could not be put to use because of non-availability of qualified staff. This included non- appointment as well as non-creation of the required posts. In one instance, orthopedic implants could not be used, as there was no framed policy for its use. An auto-analyzer could not be put to use for lack of accessories. The category wise problems in the life-cycle of different medical equipment [Figure - 2, data source] shows that in case of the equipment used in the radiology department non-availability of qualified staff, mainly radiographers and lack of infrastructure in the form of buildings, dark rooms and three phase electric connection were responsible for sub optimal utilization of the X-ray units, CT Scans and USGs. The non-availability of surgeons, trained paramedical staff and operation theatres had an adverse effect on the utilization of surgical equipment. Delay in civil works lead to non-installation of the cobalt therapy units. The problems in the purchase were seen for equipment in the wards, supportive equipment and unspecified hospital equipment. The implications of these problems were that in 25 instances the equipment could not be put to use and the public was deprived of the intended services [Table - 3]. The average period for which such equipment was lying idle was 3.91 years with a range of one and half years to fourteen years. In five instances the equipment was not purchased inspite of either paying the money of provision of funds from the government. In six cases in which the equipment was being used, there were only financial implications. Two instances of sub-optimal utilization of the equipment were noted. The non-procurement of C arm table along with the imaging system could not ensure its optimal utilization. The high level of humidity at the equipment site caused recurring malfunctioning of the CT Scan and its sub-optimal use. In nearly 50% of the instances up to Rupees 25 lakhs of funds were involved. In 17.5% cases the amount was more than one crore [Table - 4]. It is not only the purchase of major equipment that is costly but the bulk purchase of smaller instruments also leads to significant financial inputs e.g. the unauthorized diversion of funds for purchase of labor tables and drip stands amounted to Rupees 46 lakhs. The financial implications were in the form of unfruitful expenditure. Extra expenditure and locking of government funds. Unfruitful expenditure: When the equipment is bought but not utilized. It lies idle. Inspite of investment patients are deprived of essential diagnostic and curative facilities. The intended benefits of the investment are not achieved. The quality of care suffers. In two cases payment was released without receipt of equipment. Extra expenditure: Erroneous evaluation of bids and purchase of equipment at higher rates, avoidable payment of commission. Locking of government funds. The money/funds are released but there is delay in the purchase, installation and use of the equipment. The money is withdrawn in advance without requirement. There is purchase of equipment without requirement. DISCUSSION This study reiterates the huge investments made by the government on medical equipment. The equipment in the radiology department, operation theatres, special wards (ICCU, NICCU) and laboratory needs to be monitored more strictly. The mismatches in procurement of equipment and available trained staff, adequate infrastructure in the form of building, electricity etc prove to be major hindrances in the timely utilization of the costly equipment. The problems in purchase of the equipment cause financial losses as well as deprive the public of the intended services. The administrators should follow the procedures for procurement strictly. Many of the sophisticated electrical and electronic equipment are highly sensitive and require specific environmental support. The procurement of equipment, availability of trained staff and adequate infrastructure should be synchronized with respect to time. The trained staff can be recruited or the available staff can be trained. Each stage in the life cycle should be monitored carefully. The study by the program evaluation organization, planning commission has described the mismatches between staff, equipment and infrastructural support and its effect on the suboptimal utilization of the equipment.[4] Another study has noted the idle capacity in government hospitals. The ECG, X-ray units, Operation theatres, USG, vehicles were found to be idle for a period ranging from 2 to 25 years.[5] Another study has described the under-utilization of X-rays due to the non-availability of Surgeons in rural hospitals.[6] WHO has prescribed various criteria to be fulfilled before any technical equipment is purchased or accepted as a gift.[7] Some innovative methods have been tried to improve the purchase and utilization of medical equipment. The Tamil Nadu Medical Supply Corporation, an autonomous organization was established to supply drugs to all government facilities.[8] There was a significant improvement in quality, more efficient use of drugs and lower purchase rates. Its role was broadened to include medical supplies and medical equipment. The problems and the points to be considered at each stage are summarized in [Table - 5]. A well-planned national policy on acquisition, utilization and maintenance of medical equipment needs to be established. The availability of adequate funds, technical knowledge, good leadership and healthy, cost conscious administrative practices will ensure a smooth flow of medical equipment along the various stages of the life cycle. REFERENCES
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05003t2.jpg] [ms05003t1.jpg] [ms05003t3.jpg] [ms05003f1.jpg] [ms05003t4.jpg] [ms05003f2a.jpg] [ms05003f2.jpg] [ms05003t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}