
|
Indian Journal of Medical Sciences
Medknow Publications on behalf of Indian Journal of Medical Sciences Trust
ISSN: 0019-5359 EISSN: 1998-3654
Vol. 59, Num. 4, 2005, pp. 150-155
|
Indian Journal of Medical Sciences, Vol. 59, No. 4, April, 2005, pp. 150-155
Original Article
Molecular analysis of fragile X syndrome in Antalya Province
Bilgen T., Keser I., Mihci E.*, Haspolat S.**,
Tacoy S., Luleci G.
Department of Medical Genetics, *Pediatric Clinical
Genetics and **Pediatric Neurology, School of Medicine, Akdeniz
University, Antalya,
Turkey
Correspondence Address: Dr. Ibrahim Keser, Department of Medical
Genetics, School of Medicine, Akdeniz University, TR-07070 Antalya, Turkey.
E-mail:
keser@akdeniz.edu.tr
Code Number: ms05022
Abstract
Background: Detection of the (CGG)n repeats in the FMR1 gene
that cause the fragile X syndrome (FXS), has become a milestone for phenotype-genotype
correlation in FXS.
Aims: To screen the FMR1 gene CGG repeats in index cases with FXS and their family members in the Antalya Province. Setting and design: This study was prospectively conducted between January 200and March 2005 in Department of Medical Biology and Genetics, Faculty of Medicine, Akdeniz University, Antalya.
Setting and Desing: This study was prospectively conducted between
January 200and March 2005 in Department of Medical Biology and Genetics,
Faculty
of Medicine, Akdeniz University, Antalya.
Materials and Methods: A series of 132 cases from three hospitals
in Antalya Province were studied. All cases were molecularly screened
using non-radioactive Expand Long PCR method that was confirmed by Southern
blotting.
Results: Seventeen out of 132 cases were found to have a full mutation,
including three that were mosaic for premutations/full mutations. Of
the 132 cases, eight were found to have the premutation size of the CGG
repeats. The remaining 107 cases were identified as normal.
Conclusions: Due to premature ovarian failure and Fragile X premutation
Tremor/Ataxia Syndrome related with the premutation, the detection of
the premutation will provide valuable information both for clinical follow-up
and genetic counseling. In conclusion, our data suggest that expansion
of CGG repeats in the FMR1 gene can be analyzed by Expand Long PCR, an
efficient and non-radioactive method that can be used to monitor the
expansion of premutation to full mutation, which would eventually lead
to reduce the FXS prevalence.
Keywords: Antalya, CGG repeats, expand long PCR, fragile X
syndrome, FMR1 gene
The fragile X syndrome (FXS) is the most common inherited form of mental retardation.
The molecular basis of the syndrome is usually an expansion of a repetitive
CGG triplet sequence located in the 5'-untranslated region (5'-UTR)
of the FMR1 gene.[1] Rarely,
FXS results from other molecular alterations (such as point mutations or deletions)
within the FMR1 gene.[2] The
normal number of (CGG)n repeats is polymorphic and varies from 6 to
50.[3] When the expanded repeat
numbers range from 50 to 200, the allele becomes unstable in the intergenerational
transmissions and is termed as premutation.[4] The
expansion of the number of repeats above a threshold of approximately 200 repeats,
results in hypermetylation of the FMR1 promotor region and a lack of gene expression.
This allele is termed as full mutation. Alleles with >200 triplets are highly
unstable during somatic development and inheritance. Alleles that are called
'Grey zone' (approximately 50-60 triplets) are stable in somatic development,
yet their stability in transmission is unpredictable.[5] Mosaicism,
methylation and size mosaicisms, is also frequent in the FXS and closely associated
with clinical variability. Although the frequency of FXS has been estimated
to be approximately 1 in 4000 males and 1 in 6000 females, [6,7] the
frequency of premutation in the general population is ~1 in 259 females and
1 in 813 males. [8,9] The
premutation in the FMR1 gene has been reported to be associated with
premature ovarian failure.[10] On
the other hand, recently, Jacquemont et al[11] reported
fragile X premutation tremor/ataxia syndrome in a series of 26 patients, all >50
years of age, who were carriers of the fragile X premutation, and affected
by a multisystem, progressive neurological disorder. Due to increasing clinical
importance and high prevalence, the identification of the premutation carriers,
which can be detected only by direct molecular analysis is very important.[12] Here,
we aimed to detect the mutations by using an efficient and reliable PCR protocol
which enables the amplification of normal, premutated and full mutated alleles
in index cases and in members of the families with FXS, and to give effective
genetic counseling in the Antalya Province.
Materials and methods
We prospectively analyzed DNA samples isolated from the peripheral blood of 95 males and two females who had been clinically diagnosed as having FXS according to Hagerman′s Checklist (see
http://www.fragilex.org/html/checklist.htm) and 42 members in the seven families of those probands we detected to have FXS by molecular analysis (132 cases in total) between January 2000 and March 2005. Final examination and scoring of all cases was performed by two different professional physicians from the Departments of Pediatric Neurology and Clinical Genetics, School of Medicine, Akdeniz University. Index cases with a score of 13 or higher for the Hagerman′s Checklist were included in this study. Signed written consents were taken from all subjects or their parents. This study was also approved by the ethics committee of the Faculty of Medicine, Akdeniz University. The amplification primers were Fra X-Forward: 5'-ACC TCT gCA gAA ATg ggC gTT CTg gCC CTC-3' and Fra X-Reverse: 5'-CTA gCg CCg ggA gCC CgC CCC CgA gAg gT-3'. Amplification of the CGG repeat region of normal, premutated and full mutated alleles in the FMR1 gene was carried out by PCR reaction with a total volume of 25 ml, containing 200 ng of genomic DNA, 300 nM of each primer, 5% of DMSO, 5% glycerol, Expand Long PCR buffer 1,350 nM each of dATP, dCTP, dTTP, 7-deaza dGTP, and 1 U Expand Long PCR Enzyme Mix. Denaturation was performed at 95°C for 3 min. The samples were then subjected to 10 cycles of amplification (95°C for 30 s, 54°C for 30 s, 68°C for 8 min) in a thermocycler (Techne Genius). The reaction was stopped on ice, following the last denaturation for further addition of an enzyme (1 U), and continued for 30 more cycles (95°C for 30 s, 52°C for 30 s, 68°C for 8 min). The elongation time was extended for 5 sec. after each cycle in the last 30 cycles. The reaction was finalized by keeping the reaction at 68°C for 18 min, then at 4°C. The PCR product was run on 1.2% agarose gel with DIG labeled molecular weight marker (MW, VII; Boehringer Mannheim) and transferred to a positively charged nylon membrane (Boehringer Mannheim) following denaturation and neutralization procedures. DNA was cross-linked to the membrane by UV light. Blot was prehybridized for 1 h then hybridized with DIG labeled 5'-(CGG)5-3' probe in DIG Hybridization Buffer at 60°C shaking in a hybridization oven for 16 h. After washing off the membrane, the bands were detected according to the procedures described in the DIG-Luminescent Detection Kit (Boehringer Mannheim). After the incubation of CSPD at 37°C for 15 min, the membrane was exposed to Hyper ECL film (Amersham) for 10-15 min. [13,14] Normal, premutation and full mutation DNA samples were ran in each study as a control and premutations and full mutations were confirmed by Southern blotting during the initial studies.[15]
Results
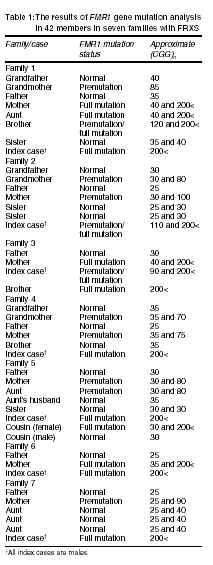
Ten of the 97 index cases were found to have full mutation by Expand Long PCR-based method. Two out of ten had both a premutation and full mutation band. A smear pattern was detected in the other eight patients. The remaining 87 cases were found to have normal sizes of the CGG repeats. Excluding seven index cases, 15 of 42 members in seven families were found to have an increase of the CGG repeats. Seven and eight of these were carriers of full mutations and premutations, respectively. One out of seven full mutation carriers had both premutation and full mutation sized bands. The remaining 20 members of the families had normal size of the CGG repeats. The results of the FMR1 (CGG)n mutation analysis in seven families are shown in
Table 1.
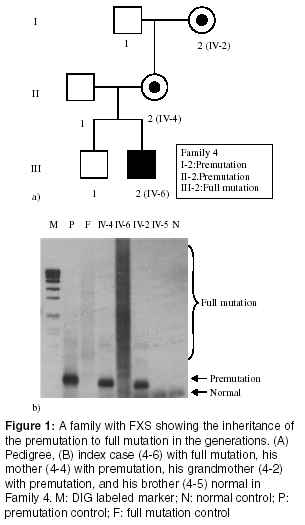
Figures 1A and
1B show the step-increasing transmission of the CGG repeats in one of the families. The premutation was transmitted with a little expansion in the premutation range from female (grandmother) (I-2) to female (mother) (II-2), then expanded to full mutation in the child (grandson) (III-2) in Family 4. Two of the mosaic patterns were transmitted from a mother with full mutation in Families 1 and 3, respectively. The remaining one, from Family 2, was observed to be transmitted by a mother with premutation
(Table 1).
Discussion
In our laboratory, the fragile X mutations had been analyzed using both
cytogenetic and genomic Southern blotting (with StB12.3 probe and double
digestion) until 2001.[15] We
also started to analyze simultaneously the fragile X mutations using the
Expand Long PCR protocol in probands and their families. In the present
study, using this protocol, we found full mutation in 10 of the 97 index
cases who have a score of 13 or higher according to Hagerman′s Checklist.
Seven full mutations and eight premutation carriers were also found among
42 members of their families. The DNA analysis of families with apparently
isolated cases of FXS indicates that even distant relatives are at risk
to be carriers. For this reason, it is imperative that members of these
families be offered FMR1 DNA studies. Our results suggest that
this technique is useful to detect the intergenerational instability of
CGG repeats in the FMR1 gene in index cases with FXS and in their
families. However, in general, the only limitation of this technique is
the smear appearance of full mutations (Figure
1B).
Although full mutations were detected mostly as a smear, the three patients
who had both full mutation and premutation-sized fragments were also identified.
These band patterns may or may not reflect the true heterogeneity of genomic
DNA isolated from peripheral blood. Also, these band patterns observed
in peripheral blood may or may not reflect the true heterogeneity of brain
and other tissues. Two of the mosaic patients were index cases with mental
retardation (Family 2-7 and Family 3-3 in
Table 1). The other one
was a member of Family 1 with mild mental retardation (Family 1-6 in
Table 1). This clinical
difference may be due to the ratio of the premutation and full mutation
in the brain neurons. Also, these findings show that all family members
with or without clinical features should be screened in the families with
FXS.
An issue for mothers with premutation alleles is the possibility of transmitting a full mutation to her offspring, as well as premature ovarian failure,[16] which we could not study in the women with premutation. In 2001, a new condition was reported in some adult males with premutation, it was called Fragile X Tremor ataxia syndrome (FXTAS).[11, 17, 18] These findings raised additional issues that should be considered by genetic counselors. In our study, no males with premutation were found, but there were three mosaic males. Due to no well-described clinical features and the high prevalence of premutation carriers, the premutation carriers must be diagnosed by an efficient molecular technique such as the PCR-based method that can identify accurately the CGG repeat size, and that we used in the present study. Two male fetuses were prenatally diagnosed with this method, one had a normal allele and the other carried a full mutation. These results were confirmed by Southern blot using Eag I/ Eco RI double digestions. We started the screening of the general population for the prevention of the birth of a child with FXS or beta-thalassemia in Antalya. The index cases that were found to be normal for the CGG repeats will be screened to detect other molecular alterations (such as point mutations and deletions) in the FMR1 gene. We believe that the recording and following of families with FXS will provide prenatal diagnosis and the usage of a possible treatment opportunity in the future. As a result, our data show that all the members with/without clinical findings of FXS in the families with FXS should be screened by the PCR-based method to follow the transmission of the CGG repeats and to give correct genetic counseling to families.
Acknowledgment
This study was supported by the Research Foundation of the Akdeniz University.
References
| 1. | 1. Brown WT, Nolin S, Houck G Jr, Ding X, Glicksman A, Li SY, et al. Prenatal diagnosis and carrier screening for fragile X by PCR. Am J Med Genet 1996;64:191-5. Back to cited text no. 1 [PUBMED] |
| 2. | 2. Castellvi-Bel S, Sanchez A, Badenas C, Mallolas J, Barcelo A, Jimenez D, et al. Single-strand comformation polymorphism analysis in the FMR1 gene. Am J Med Genet 1999;84:262-5. Back to cited text no. 2 |
| 3. | 3. Kallinen J, Heinonen S, Mannermaa A, Ryynanen M. Prenatal diagnosis of fragile X syndrome and the risk of expansion of a premutation. Clin Genet 2000;58:111-5. Back to cited text no. 3 |
| 4. | 4. Willemsen R, Oostra BA. FMRP detection assay for the diagnosis of the fragile X syndrome. Am J Med Genet 2000;97:183-8. Back to cited text no. 4 |
| 5. | 5. Dobkin C, Ding X, Li S, Houck G Jr, Nolin SL, Glicksman A, et al. Accelerated prenatal diagnosis of fragile X syndrome by polymerase chain reaction restriction fragment detection. Am J Med Genet 1999;83:338-41. Back to cited text no. 5 |
| 6. | 6. de Vries BB, van den Ouweland AM, Mohkamsing S, Duivenvoorden HJ, Mol E, Gelsema K, et al. Screening and diagnosis for the fragile X syndrome among the mentally retarded: An epidemiological and psychological survey. Collaborative Fragile X Study Group. Am J Hum Genet 1997;61:660-7. Back to cited text no. 6 |
| 7. | 7. Turner G, Webb T, Wake S, Robinson H, et al. Prevalence of fragile X syndrome. Am J Med Genet 1996;64:196-7. Back to cited text no. 7 [PUBMED] |
| 8. | 8. Rousseau F, Rouillard P, Morel ML, Khandjian EW, Morgan K. Prevalence of carriers of premutation-size alleles of the FMRI gene - and implications for the population genetics of the fragile X syndrome. Am J Hum Genet 1995;57:1006-18. Back to cited text no. 8 [PUBMED] |
| 9. | 9. Dombrowski C, Levesque S, Morel ML, Rouillard P, Morgan K, Rousseau F. Premutation and intermediate-size FMR1 alleles in 10572 males from the general population: loss of an AGG interruption is a late event in the generation of fragile X syndrome alleles. Hum Mol Genet 2002;11:371-8. Back to cited text no. 9 |
| 10. | 10. Allingham-Hawkins DJ, Babul-Hirji R, Chitayat D, Holden JJ, Yang KT, Lee C, et al. Fragile X premutation is a significant risk factor for premature ovarian failure: The International Collaborative POF in Fragile X study - preliminary data. Am J Med Genet 1999;83:322-5. Back to cited text no. 10 [PUBMED] [FULLTEXT] |
| 11. | 11. Jacquemont S, Hagerman RJ, Leehey M, Grigsby J, Zhang L, Brunberg JA, et al. Fragile X premutation tremor/ataxia syndrome: Molecular, clinical, and neuroimaging correlates. Am J Hum Genet 2003;72:869-78. Back to cited text no. 11 |
| 12. | 12. Toledano-Alhadef H, Basel-Vanagaite L, Magal N, Davidov B, Ehrlich S, Drasinover V, et al. Fragile-X carrier screening and the prevalence of premutation and full-mutation carriers in Israel. Am J Hum Genet 2001;69:351-60. Back to cited text no. 12 |
| 13. | 13. Hecimovic S, Barisic I, Muller A, Petkovic I, Baric I, Ligutic I, et al. Expand Long PCR for fragile X mutation detection. Clin Genet 1997;52:147-54. Back to cited text no. 13 |
| 14. | 14. Uyguner ZO, Wollnik B, Kayserili H, Tükel T, Basaran S, Apak MY. Establishment of a nonradioactive molecular diagnosis of fragile X syndrome. Turk J Med Sci 2000;30:253-60. Back to cited text no. 14 |
| 15. | 15. Keser I, Luleci G, Alkan M. The results of molecular and cytogenetic analysis in 6 families with fragile-X syndrome in Turkey. Marmara Med J 2000;13:7-10. Back to cited text no. 15 |
| 16. | 16. Sherman SL. Premature ovarian failure in the fragile X syndrome. Am J Med Genet 2000;97:189-94. Back to cited text no. 16 |
| 17. | 17. Tassone F, Hagerman RJ, Taylor AK, Gane LW, Godfrey TE, Hagerman PJ. Elevated levels of FMR1 mRNA in carrier males: A new mechanism of involvement in the fragile-X syndrome. Am J Hum Genet 2000;66:6-15. Back to cited text no. 17 |
| 18. | 18. Hagerman RJ, Hagerman PJ. The fragile X premutation: Into the phenotypic fold. Curr Opin Genet Dev 2002;12:278-83. Back to cited text no. 18 |
Copyright 2005 - Indian Journal of Medical Sciences
The following images related to this document are available:
Photo images
[ms05022f1.jpg]
[ms05022t1.jpg]
|

{kind=link}
{kind=link}