 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
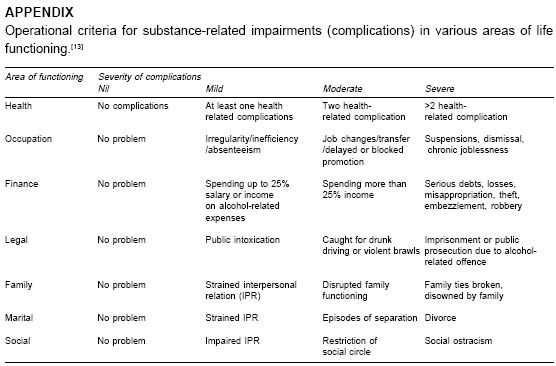
Indian Journal of Medical Sciences, Vol. 59, No. 7, July, 2005, pp. 283-291 Original Article Substance-dependent women attending a de-addiction center in North India: Sociodemographic and clinical profile Grover S., Irpati A.S., Saluja B.S., Mattoo S.K., Basu D. Merseycare NHS Trust Hesketh Centre, 51-55 Albert Road Southport - PR9 0LT England Code Number: ms05044 ABSTRACT Background: Treatment-seeking is limited in women substance abusers. Studying the sociodemographic and clinical profile of treatment-seeking substance-dependent women can help us to understand the problem better and respond appropriately in terms of primary and secondary prevention strategies.Aim: To study the sociodemographic and clinical profile of women attending a de-addiction centre in North India. Design and Methodology: Retrospective structured chart review of 35 women substance abusers. Results: The results indicated that a typical subject was urban (86%), married (63%), nuclear family (60%), based housewife (57%), educated up to school completion (54%), and having poor social support (57%). The common substances were opioids (60%), followed by alcohol (17%), and tobacco and benzodiazepines (11.5% each). The mean age at onset of substance use was 30.5 years, the mean duration of use was 9 years and mean duration to develop dependence was 5.5 years. The common reasons for initiating use were medical (63%) and curiosity (34%). Comorbidity profile was: physical illness (34%), psychiatric illness (23%) and dependence on another substance (14%). Only 20% had a family history of substance dependence. The social impairment ranged from 77% for social to 40% for financial and none for legal aspects. A typical subject had followed up 4.2 times in 8.4 months, while 54% were abstaining, 40% were continuing their substance dependence at the last follow up. Conclusions: The results suggest that the development of substance dependence in women is a combination of genetic, personal, and social vulnerability factors, including the drug culture of the social milieu and the poor social support. Comorbidity and impairment are common features. Keywords: substance dependence; women Although gender differences in drug abuse have narrowed over the last few decades, [1],[2],[3] substance abuse in women still attracts greater social stigma than in men, with attendant efforts by women to hide the problem and by the caregivers in not recognizing the problem, thereby limiting treatment-seeking. [4] , [5] MATERIAL AND METHODS The study was conducted at the Drug De-addiction and Treatment Centre (DDTC) in a tertiary-care medical centre with a large catchment area comprising of several states in North India. Most patients come by self-referral or family-referral, whereas some are referred from other hospitals or other departments of our Institute. The DDTC services include outpatient, inpatient, laboratory, aftercare, liaison with other governmental and nongovernmental agencies, and self-help groups.The cohort for this study consisted of all women patients registered at the DDTC between September 1978 and December 2003 (a little over 26 years). Substance dependence was diagnosed as per ICD-9 [11] until December 1992 and later ICD-10 [12] by a consultant psychiatrist after direct interview with the patient and her relatives. Following detailed evaluation, the treatment consisted of detoxification, symptomatic treatment, treatment of medical complications, if any and psychosocial counselling of patients and their families. Regular (usually monthly) follow ups were done by a psychiatrist when patients′ drug use profile, social and occupational functioning, and physical and psychological problems were monitored and documented. For this chart-review study, we found that for the 56-women subjects registered (seven in 2003), the case records were available only for 35 subjects. Measures The following measures were considered in this study. Socio-demographic information profile A semi-structured proforma was used to record sex, age, marital status, educational level, occupation, income, family type, religion, and locality. One variable named ′family/social support system′ was added to this section. ′Poor support′ was rated when there was either unavailability of, or lack of assistance from, key care-giving and supervising figures in the family (usually spouse, but also parents, sibs or children), or in society (peer group, colleagues, job supervisor, self-help groups, religious-spiritual affiliations, etc.). ′Good/fair′ support was rated when there was availability and assistance from at least one member each from both these sources. As the social support of an individual could vary over time, the inference about the same was drawn from cumulative evaluation of the patient, from the first contact to the last contact. Information on clinical and substance-use profile This included type of predominantly used substance, duration of dependence (onset marked from the year in which the patient first met criteria for dependence as per ICD-9 or 10), relapses, treatments, and hospitalizations in the past (before the index treatment episode), detailed physical and psychiatric comorbidity, and other substance use. The information about the physical and psychiatric comorbidity was inferred from the history, clinical and laboratory evaluation, and monitoring of the patient throughout the contact period. Impairment in various areas of functioning Four levels of drug-related complications were operationalized (Appendix). [13] These covered areas of functioning such as health, occupation, finance, family, marital, legal and social areas. The severity of complications at the first presentation (nil, mild, moderate and severe) was extracted from the case records using a standardized guideline as mentioned in the Appendix. Status at last follow up Abstinence, lapse or relapse was considered as the primary outcome measure. Abstinence was defined as no substance intake. Lapses were defined as using the substance less than that for relapse. Relapse was defined as re-emergence of substance dependence as per the ICD-9 or 10. Duration of follow up -This was calculated in number of months from first visit to the last visit to the hospital. RESULTS Sociodemographic profile [Table - 1] Only 8 (22.9%) subjects had a lifetime history of comorbid psychiatric disorders, the most common being ′Neurotic, Stress-related and Somatoform disorders′(ICD-10
codes F40-48, present in five cases). Five subjects, dependent on two or more
substances included four subjects who were co-dependent on opioids and benzodiazepines. DISCUSSION The current study was a retrospective chart review with the aim of studying the sociodemographic and clinical profile of women presenting to a de-addiction centre of a tertiary care hospital. The profile of treatment seekers can help the treatment agencies to prepare themselves in managing such cases.Sociodemographic profile Over the 26 years, 56-women subjects registered, with seven reporting in the last 1 year indicating an increase in recognition and need for treatment. Increase in the number of cases in recent years and most cases coming from urban nuclear families with poor social support reflect the transitional nature of Indian society - alterations in lifestyle and the changing roles increase the stress and bring many new problems, drug abuse being one of them. Four out of 35 subjects belonging to medical profession reflect the easy availability leading to high vulnerability of this profession. Approximately half of the subjects having completed schooling are in line with the findings of multicentric Rapid Assessment Study, which found more educated women drug abusers. [14] Clinical profile Opioids The majority of the sample were opioid dependent, most of them using IV pentazocine, although some preferred dextropropoxyphene. Only one woman was using smack (street heroin). Use of IV opioids in 42% of subjects is in line with the previous reports from other parts of India. [10] The most common antecedent for opioid use was pain leading to consultation with the local doctors who prescribed opioids. Only one of the subjects had antecedent depression. These findings support Ganguly et al.,[9] whose ethnographic study from Rajasthan reported that many of the opioid-dependent women had graduated to dependence only after initial use of opioids as medication. Further, in our study the most common opioid was pentazocine rather than heroin; the reason for this difference could be the geographic location or the type of sample (in the UNDCP study, [10] the subjects were nontreatment seekers). Overall, the findings of this study suggest that opioid analgesics should be used for the shortest possible duration and only for specific indications, rather than as a general analgesic. Alcohol Out of the six subjects using alcohol, four came from families where a key member was drinking, including three who were introduced to alcohol by their husbands; these findings are in line with the other studies from India. [8] In all the subjects, reason for starting alcohol was curiosity. None of the subjects self-referring reflects either, nonrecognition of their dependence, or avoiding treatment seeking due to social stigma. Three out of six subjects had associated complications. None of the subjects had family history of drug dependence or other substance abuse. Only one subject had antecedent depression. Benzodiazepine Only four subjects were dependent on benzodiazepines; three having become dependent following medical use either for depression or for adjustment problems with the spouse, and the duration to develop dependence was shorter. Despite the small numbers, these findings suggest that benzodiazepines should be either unused or used for the shortest possible duration. Nicotine Most of our women nicotine users came from sociocultural background where it was acceptable and none sought treatment at their own initiative. Impairment/burden The majority of the sample had only mild impairment in most of the domains, probably indicating that the subjects in the sample were less-severely ill. Outcome Most of the subjects abstaining from the drugs after appropriate treatment may appear to suggest that appropriate treatment helps most of the subjects to leave the drugs; however, the short follow up does not support this finding very strongly, while a positive correlation between abstinence and the number of follow ups indicates the need to follow up these subjects for as long as possible. Limitations of the study The small potential sample size of this study was made still smaller by the availability of case notes on only 35 out of the 56 identified cases. The study was based on a retrospective chart review where data had to be inferred from the recorded facts/narratives. Some of the instruments and definitions used for some of the assessments (e.g. social support, impairment, burden, and outcome) were study/centre specific and have not been evaluated for their reliability. Various substance-subgroups were too small for any definitive conclusions. Some of the statistically significant correlations between some of the clinical and outcome variables could be a possible chance occurrence. Lastly, being based on a single centre catering to a certain geographic area, the study did not represent the diverse (substance use) cultures of India. The findings of this research can be generalized only within these limitations. REFERENCES
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05044t3.jpg] [ms05044t1.jpg] [ms05044ap.jpg] [ms05044t2.jpg] |
| |||||||||

{kind=link}