 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 59, No. 8, August, 2005, pp. 337-346 Original Article Elisa kit evaluation for IGG and IGM antibodies to A-60 tubercular protein antigen Kalantri Y, Hemvani N, Bhatia GC, Chitnis DS Department of Microbiology and Immunology, Choithram
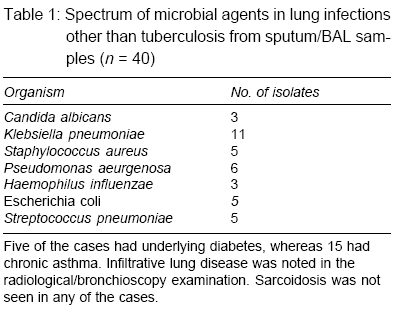
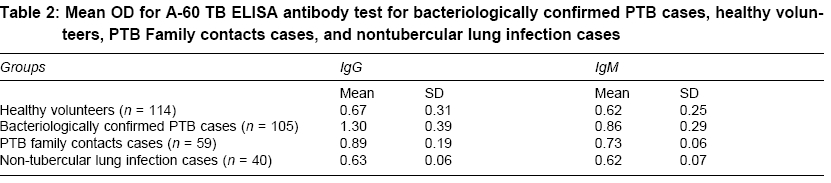
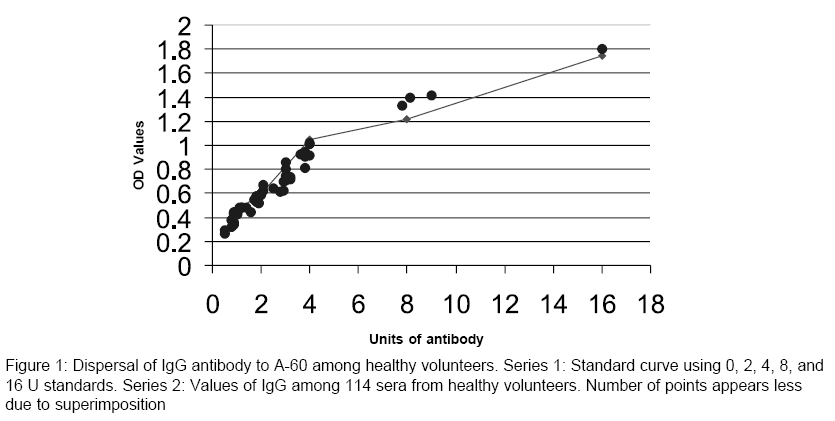
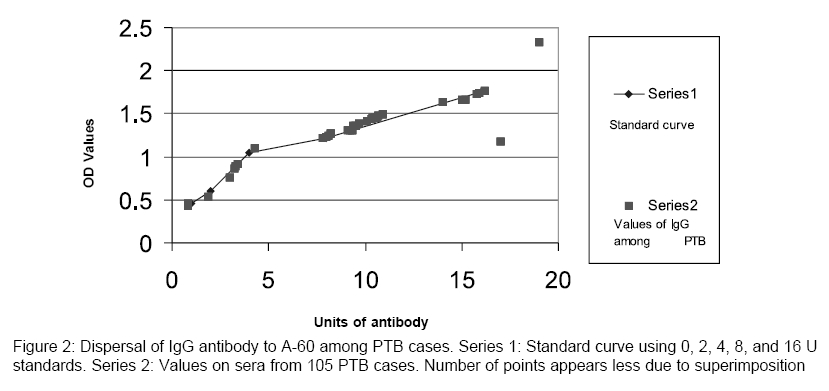
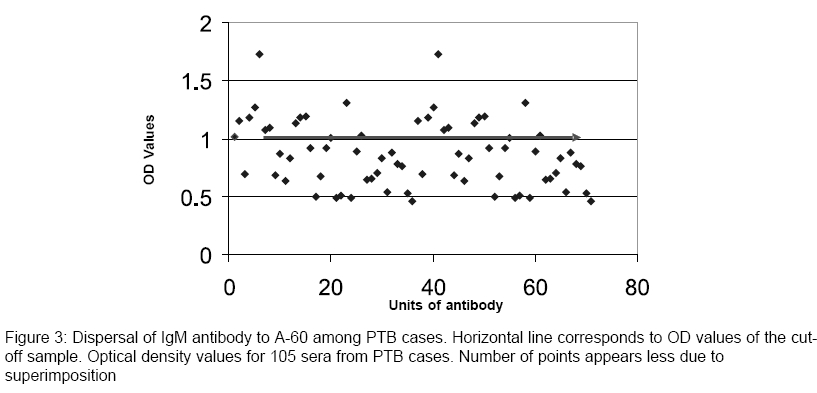
Hospital and research Centre, Indore Code Number: ms05051 Abstract AIMS: The purpose of this study is to evaluate the A-60 antigen-based enzyme-linked immuno sorbent assay (ELISA) test for its sensitivity, specificity, and other related statistical parameters. Keywords: A-60 antigen; ELISA; IgG; IgM; tuberculosis India with 14 million cases of tuberculosis carries one-third of the global load of the disease and it is feared that 1000 people die of tuberculosis everyday in India. The early diagnosis of the disease could be the major step in control of the disease. Smear examination and in-vitro culture of tubercle bacilli has remained the golden standard. However, in practice[1] the smear sensitivity remains around 30%. The culture requires a long-waiting period and has shortcomings. Polymerase chain reaction is claimed to be more sensitive than bacteriology, but demands high-level skill, expensive setup, and reagents. Further, all the above methods demand sample from site of infection and in many extra pulmonary situations may not be possible. Hence, serological diagnosis has attracted the attention of laboratories all over the world. An array of commercial kits to detect antibodies against A-60, 38 kDa and other antigens such as ES-31 antigen, KP-90 antigen, Lipoarabinomannan, and many more antigens have been largely evaluated in the Western countries and the threshold value has been setup on the basis of the Western population, where endemicity is low and mass Bacillus Calmette Guerin (BCG) vaccination not practiced. Hence, local evaluation before marketing the kits in India is required. The A-60 antigen-based kit was selected for evaluation, because it has been used widely in the country as evident with the Indian literature. [2],[3],[4],[5],[6],[7],[8],[9],[10],[11],[12] The antigen A-60 complex is a major mycobacterial antigen and the main component of reference tuberculin RT23.[13] A-60 antigen is extracted from Mycobacterium bovis strain BCG. It is composed of proteins, carbohydrate, and lipid in roughly equal amount.[14],[15] The purpose of the present study is to evaluate the A-60 antigen-based enzyme-linked immuno sorbent assay (ELISA) kit using sera from normal local population, bacteriologically proved pulmonary tuberculosis (PTB) cases, nonsymptomatic family contacts of PTB cases, and nontubercular lung infection cases to evaluate sensitivity, specificity, efficiency, reproducibility, and predictive value. The serological diagnosis can be of value for extra-PTB. However, bacteriologically confirmed cases of extra-PTB are not easily available and hence, only bacteriologically confirmed cases of PTB were included in the present study for the test evaluation. Methods The four groups of cases included in the present study were healthy volunteers, bacteriologically confirmed cases of PTB, healthy contacts of PTB cases, and cases of lung infections other than tuberculosis. Healthy volunteers : healthy voluntary blood donors from Indore city and the adjoining area who came for blood donation from September to December 2003 at the Blood Bank of Choithram Hospital and Research center were included as normal population. All the 114 volunteers (89 men and 25 women) were in the age group of 21-50 years and neither had history of any notable infection in the past 2 years, nor had symptomatic tuberculosis in the lifetime. Tuberculin test, however was not carried out on them. Bacteriologically confirmed cases of PTB : The exclusion criteria were PTB cases on chemotherapy and new cases not willing for informed consent. The symptomatic phase before coming to the clinic ranged from 1 month to 1 year. The blood samples for the serology were collected within 1 week of documentation of AFB in sputum and before starting chemotherapy. The group comprised of 70 men and 35 women. The PTB status was further confirmed by AFB culture on Lowenstein-Jensen medium after alkali concentration of sputum samples. Family contacts of PTB cases : Cases of lung infections other than tuberculosis : Tuberculin test was carried out on all subjects from PTB group, family contacts, and nontubercular lung diseases group using 5 U purified protein derivative (PPD) (Span diagnostics, India). Sera samples from all the subjects were given code numbers and stored at -700°C till the day of testing for the antibody test. Decoding was done at the time of data analysis. Commercially available IgG and IgM antibody test manufactured by Anda Biologicals (67067 STRASBOURG Cedex, France) was used in the study. The test detects antibodies to A-60 antigen coated over the wells. The ELISA test was carried out as described in the manufacturer′s protocol. The sera samples and the kit reagents were allowed to come to room temperature before the test. Positive and negative controls provided in the kit were run for every batch of ELISA test. The sera samples were diluted 1 : 100 in the sample diluent. The diluted samples and controls added (100 ml) to the wells and incubated at 370°C per 1 h. The wells washed five times before adding anti human IgG- or IgM-peroxidase conjugate. After 30 min at 370°C the wells washed again five times and 100 ml tetramethylbenzidine substrate was added. The reaction was stopped by the addition of 100 ml H2SO4 after 15 min incubation at 370°C and absorbance measured at 450 nm using MRX-ELISA (Dynex, USA) plate reader. The hospital ethical committee had approved the study and informed consents from patients and volunteers were taken before including them in the study. Statistical methods IgM cut-off sample and IgG 4 U/ml reference standard provided in the kit were run in duplicate consecutively (weekly) for 10 weeks to plot the variation with reference to 1 and 2SD. For making scatter diagram for sera from healthy volunteers and from PTB cases, optical density (OD) values for the sera were plotted to study dispersal of the range. Optical density values for sera from PTB cases, healthy volunteers, family contacts, and nontubercular lung cases were used to determine sensitivity, specificity, and efficiency using the standard formulae.[16] Predictive values were calculated as a measure of value of a test in relation to the prevalence of disease in the population.[16] Differences in OD values of sera from various groups were checked for statistical significance, using two tailed, two sample unequal variance t -test.Results Mycobacteria were isolated from all the 105 sputum samples from PTB cases. Ninety-nine of the isolates were Mycobacterium tuberculosis complex (Niacin test positive), whereas six were mycobacteria other than tuberculosis (MOTT). None of the sputum samples from nontubercular lung infection cases revealed the growth of mycobacteria. The microbial spectrum of the nonmycobacterial agents from sputum/BAL samples in the group is depicted in [Table - 1]. Five of the cases had underlying diabetes, whereas 15 had chronic asthma. Infiltrative lung disease was noted in the radiological/bronchoscopy examination. Sarcoidosis was not seen in any of the cases. Tuberculin test was positive among 84/105 PTB cases, 12/59 contacts of PTB cases, and four of the nontuberculosis lung infection cases. Mean OD values in ELISA test for A-60 antibodies for sera from PTB cases, healthy volunteers, family contacts of PTB cases, and nontubercular lung infection group are given in [Table - 2]. Differences in mean OD among sera from healthy volunteers and PTB cases both for IgG and IgM were highly significant in two tailed, two sample unequal variance t -test ( P < 0.001 and 0.001, respectively). Similarly, differences among mean OD values for sera from healthy volunteers and family contacts of PTB cases were also statistically significant for IgG and IgM antibody ( P values < 0.001 and 0.002, respectively). However, differences in mean OD values for healthy volunteers and the group of non-tubercular lung infection were not significant for IgG and IgM antibody to A-60 antigen ( P = 0.44 and 0.97, respectively). The mean +2SD OD value for IgG and IgM among sera from healthy volunteers was considered as threshold to report as positives. Scatter diagram for IgG antibody to A-60 among healthy volunteers is displayed in [Figure - 1]. Standard curve using OD values for 2, 4, 8, and 16 units of standard IgG against OD values is shown in the background and it is evident that only four sera among healthy volunteers were outliers (value above 400 U/ml considering 1 : 100 dilution of the serum). Scatter diagram for IgG values among PTB cases is shown in [Figure - 2]. Eighty-four samples had IgG levels above 4 U (for 1 : 100 serum dilution) (values superimposed over ten points). In case of IgM, antibody levels were above the threshold for 30 sera [Figure - 3]. The scatter diagram also supports the threshold levels setup on the basis of mean +2SD values for IgG and IgM antibody test. Positivity, sensitivity, and specificity for IgG and IgM antibody: IgG and IgM positivity in various groups is shown in [Table - 3]. Eighty-four IgG positives and 30 IgM positives in PTB group were considered as true positive, whereas the positive samples among healthy volunteers and contact of PTB were considered as false positives. Twenty IgG negative and 75 IgM negative samples in PTB group were considered as false negatives. The sensitivity for IgG antibody test was 80%, specificity was 95.8%, efficiency 90.5%, and positive predictive value 90.3%. In case of IgM, antibody sensitivity was as low as 28.6% but specificity was 95.7%, efficiency was 73.6%, and positive predictive value was 77%. Reproducibility check is essential as a quality control measure. The IgM reference cut-off was run weekly for ten consecutive weeks and the dispersion was studied. Almost all values lay within 1SD and only one value was closer to 2SD. In case of IgG, 4 U reference standard was run weekly for ten consecutive weeks and the results were within 1SD for all the tests, whereas only two points were proximal to 2SD. Therefore, good reproducibility was observed for IgG and IgM controls. Discussion Comorbidity of HIV and tuberculosis is well known. In the present series, the PTB cases included were part of the anonymous HIV surveillance program and three of the 105 subjects were HIV antibody reactive (not mentioned in results). Tuberculin test is an indicator of cell-mediated immune response to tuberculosis. Eighty-four of the bacteriologically confirmed cases were positive in tuberculin test and the same number of the sera samples were positive for IgG antibody. However, 15 of them showed discrepancy, that is, antibody test positive but tuberculin test negative and vice versa. It also needs to be pointed out that 12 subjects among PTB contacts and four cases of nontubercular lung disease cases were tuberculin test positive but negative for IgG and IgM antibody to A-60. The contacts of PTB cases included in the study were spouses of the index PTB cases and five of them were IgG positive, whereas three were IgM positive. The positivity could be due to exposure resulting in nonsymptomatic infection or the immune response without getting active infection. Further follow up in relation to development of active infection was not done. It would have been interesting to study IgG and IgM levels to A-60 antigen among treated PTB cases. However, only 24 treated cases were available for follow up (results not included in ′result′part). None of them had IgM antibody to A-60 above cut-off, whereas IgG antibody was positive for all the cases. In six of the cases, IgG level was reduced compared to the initial value before anti-tubercular treatment while IgG level was found to increase in 18 cases. Reduction in IgG level could be due to the waning of the antigen following effective therapy and increased IgG level correlated with the continued immune response subsequent to the initial IgG level. Sero-diagnosis of tuberculosis using various antigens-based ELISA tests has been reviewed by Bhatia et al.[10] The review mentioned A-60-based IgG antibody test to be more sensitive and specific than IgM antibody. The 38 kDa antigen-based tests were reported to be specific but less specific. Uma et al.[17] reported sensitivity as 61% for IgG and only 10% for IgM antibody using 38 kDa antigen and Mathai et al.[18] compared five different antigens-based commercial kits and the sensitivity varied from 46 to 68%. Meena et al.[3] reported A-60- and LPS-based tests to be more sensitive and specific than 38 kDa and KP-90-based ELISA tests. It appears that the Indian experiences are more with A-60 antigen-based kits. [2],[3],[4],[5],[6],[7],[8],[9],[10],[11],[12] The threshold values used by Munshi et al.[9] was 200 U and Maheshwari et al.[6] had selected 250 U as threshold. In the present study, threshold had to be raised to 400 U. Therefore, setting up of threshold values for the individual laboratory based on the local population is required for adequate sensitivity and specificity. The duration of illness and the age group also need to be considered for the negative antibody tests. Ahmed et al.[2] pointed out lower positivity for age group 1-14 years and duration of less than 3 months in case of tuberculous lymphadenitis. The class of the antibody is also an important factor. Immunoglobulin G holds the great promise in diagnosis of active tuberculosis both in children and in adults.[10] Sensitivity and specificity for IgG antibody to A-60 was found to be in the range of 75-100% in various other Indian reports. [2],[3],[4],[5],[6],[7],[8],[9],[10],[11],[12] However, proper evaluation, setting up of thresholds, and reproducibility study was lacking in most of the studies. The IgM antibody is the first to appear for any antigen and therefore could be expected to be of diagnostic value for the recent tuberculosis. However, in case of IgM antibodies test, the sensitivity was low (28.5%) in the present study. This possibly could be due to inclusion of PTB cases with a symptomatic history of 1-12 months. As a result of longer duration of infection, the IgM antibodies might have declined in the proportion of PTB cases. Longer incubation period in case of tuberculosis may result in decline of IgM before symptoms appear. However, the IgM antibody appears to be less sensitive as evident in the present study and also has been reported by others.[6],[10],[12] Bhatia et al.[10] reported IgG sensitivity of 94% and IgM sensitivity of only 33% in extra-PTB, whereas Maheshwari et al.[6] observed IgG sensitivity of 75% and IgM sensitivity of 37.5% in tuberculoma cases. A limitation of the present study has been noninclusion of extra-PTB cases. Hence, the multicentric trials on the diagnostic utility of the test on cases of extra-PTB are suggested. To conclude, the threshold value setup for IgG antibody to A-60 antigen was 400 U/ml. The IgG antibody test had sensitivity of 80% and specificity of 95.8%. The sensitivity for IgM antibody was low (28.6%), although the specificity was high (95.7%). The ELISA kit also showed good reproducibility. Acknowledgments We are thankful to the management of Choithram Hospital and Research Center Indore (MP) for providing the facility for the research work. Special thanks to Dr. Santosh Chobe and Dr. B. S. Chadda from Choithram Dispensary, Indore for providing the blood samples of PTB cases.References
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05051t1.jpg] [ms05051f1.jpg] [ms05051t2.jpg] [ms05051f2.jpg] [ms05051t3.jpg] [ms05051f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}