 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
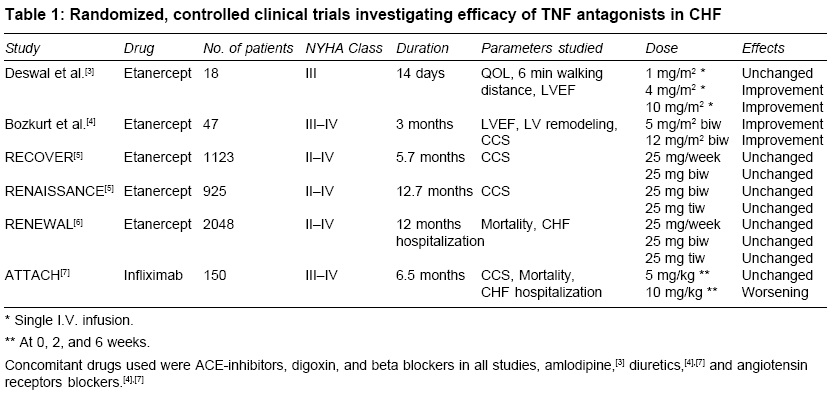
Indian Journal of Medical Sciences, Vol. 59, No. 8, August, 2005, pp. 363-366 Practitioners section Current status of TNF blocking therapy in heart failure Gupta S, Tripathi CD Department of Pharmacology, VMMC & Safdarjung Hospital, New Delhi Code Number: ms05056 ABSTRACT Recent experimental studies have shown that tumor necrosis factor alpha (TNF-α) has deleterious cardiovascular effects. Tumor necrosis factor alpha antagonists bind to TNF-a and functionally inactivate this cytokine and thereby reverse some of these effects. Various clinical studies of TNF-α antagonists have reported conflicting results. The present review analyses all reported clinical trials of TNF-α antagonists in congestive heart failure (CHF). The effect of these agents on clinical composite score, CHF hospitalizations, and mortality were compared. Early clinical studies of blocking TNF in patients with heart failure demonstrated promising results. However, recent large-scale, placebo-controlled trials have failed to show any improvement in the clinical status of heart failure. There have in fact, been some reports of worsening of heart failure with these agents. It may be concluded that TNF-α antagonists could adversely affect the clinical condition of patients with moderate to severe heart failure. Keywords: antagonist; heart failure; TNF-α. Serum levels of tumor necrosis factor alpha (TNF-α) are elevated in patients with heart failure and this overproduction is largely of cardiac origin. The magnitude of increase is directly proportional to the severity of disease. These elevated levels of TNF-α may contribute directly to progression of heart failure.[1] Tumor necrosis factor alpha can cause pathological changes that are characteristic of failing human heart such as ventricular remodeling, interstitial fibrosis, and cardiomyocyte apoptosis.[2] Tumor necrosis factor alpha also has established negative inotropic effects. These facts indicating that TNF-α is a deleterious factor in heart failure generated a lot of enthusiasm for the use of anti-TNF therapy in the management of heart failure. Several in-vitro and in-vivo experiments also demonstrated that TNF-α blocking therapy might improve cardiovascular function by reversing some of the deleterious effects of TNF-α. However, clinical trials of TNF-α antagonists for treatment of heart failure have reported controversial results. The clinical data on TNF blockers have been reviewed in patients with congestive heart failure (CHF) to answer the unresolved questions about the role of TNF-α in heart failure and important concerns about the efficacy and safety of using TNF-α antagonists have also been reviewed. At the time of our review, two TNF-α antagonists, Etanercept, and Infliximab were approved for clinical use, although for different indications. Etanercept is a recombinant, soluble TNF type 2 (p75) receptor fusion protein used to treat rheumatoid arthritis and psoriatic arthritis. Infliximab is a chimeric monoclonal antibody against TNF-α and is used to treat rheumatoid arthritis in patients unresponsive to methotrexate, and Crohn′s disease. Neither product is indicated for the prevention nor treatment of heart failure. Randomized trials of anti-TNF-α therapy in CHF were identified by performing a systematic review of the literature. The search yielded six eligible trials. There were slight variations in the target population, individual trial design, and inclusion and exclusion criteria. A preliminary clinical study by Deswal et al.[3] evaluated the safety and efficacy of Etanercept in patients with advanced heart failure. Eighteen patients with NYHA Class III CHF were randomized into a double blind dose escalation study. A single intravenous infusion of Etanercept was sufficient to lower levels of biologically active TNF-α and lead to improvements in the quality of life (QOL), 6-minute walking distance, and left ventricular ejection fraction (LVEF) [Table - 1]. However, the results of this study must be considered as provisional because of the relatively small sample size and short duration of follow up (14 days). Another randomized, double blind multidose trial by the same group followed in which 47 patients were treated with biweekly subcutaneous injections of Etanercept or placebo for 3 months.[4] In this pilot study, treatment with Etanercept was well tolerated and was reported to improve cardiac function and clinical status in advanced CHF. After this, two multicenter clinical trials using Etanercept were initiated in patients with NYHA II-IV heart failure. The trial in North America, entitled randomized Etanercept North American strategy to study antagonism of cytokines (RENAISSANCE), and the trial in Europe and Australia, entitled research into Etanercept cytokine antagonism in ventricular dysfunction (RECOVER) were both QOL trials that used a clinical composite as the primary end point.[5] The clinical composite score (CCS) classifies patients as better, worse, or the same after a clinical intervention, on the basis of the patient′s and the physician′s assessment at the end of the study. Both trials had parallel study designs but differed in the doses of Etanercept that were used in the two studies: RENAISSANCE used doses of 25 mg, twice a week (biw) and 25 mg, three times a week (tiw), whereas RECOVER used doses of 25 mg once a week (qw), and 25 mg biw. A third trial, which used the pooled data from the RENAISSANCE (biw and tiw dosing) and RECOVER (biw dosing only), termed randomized Etanercept worldwide evaluation (RENEWAL), had a primary end point of all cause mortality and hospitalization for heart failure. Preliminary analysis of the data showed no benefit for Etanercept on the clinical composite end point in RENAISSANCE and RECOVER or a benefit for Etanercept on all cause mortality and heart failure hospitalization in RENEWAL.[6] Hence, these trials were stopped early. The anti-TNF therapy against congestive heart failure (ATTACH) trial was a Phase-II study in 150 patients with the primary end point of CCS. Analysis of the completed trial data showed that there was a dose-related increase in death and hospitalizations due to heart failure with Infliximab compared with placebo at 14 and 28 weeks [Table - 1].[7] Kwon et al.[8] examined spontaneous adverse event reports to the US food and drug administration′s (FDA) MedWatch system for evidence that TNF antagonists can exacerbate heart failure or promote new onset of heart failure. Etanercept and Infliximab were prescribed for the management of rheumatoid arthritis, Crohn′s disease, psoriatic arthritis, and juvenile rheumatoid arthritis. The analysis of data on 47 patients who developed heart failure while receiving long-term (up to 3 years) TNF antagonist therapy showed that 81% had never experienced heart failure before taking TNF antagonists. Half of the patients with new onset of heart failure had no identifiable heart failure risk factors. Resolution or improvement of heart failure after withdrawal of TNF antagonists and administration of heart failure treatment in nine younger patients (<50 years of age) indicates a causal connection. Despite the encouraging results of initial small pilot trials with Etanercept, the results of large-scale multicenter trials do not demonstrate any clinical benefits, and in fact suggests that TNF blocking therapy might adversely affect the course of patients with CHF in a dose-dependent manner. The reason why this TNF-a antagonism adversely affects the clinical status in CHF is not clear. By complexing with circulating TNF-α, and thereby retaining it with the circulation, Etanercept may prolong exposure of cardiac tissue to TNF-α and potentially lead to cardiac toxicity.[9] Infliximab can cause cell lysis in the presence of complement when exposed to cells expressing transmembrane TNF-, and produce an effect that would be undesirable if it occurred in cardiomyocytes in patients with CHF.[10] Animal experiments and early clinical studies of blocking TNF in patients with heart failure demonstrated promising results. However, large scale, randomized, placebo controlled trials of TNF-α antagonists for treatment of heart failure were stopped early because they failed to demonstrate an improvement in the clinical status of heart failure or mortality. The discouraging results of clinical trials and case reports have important pragmatic implications. The prescribing information for Etanercept and Infliximab now suggests that physicians exercise caution in the use of these agents in patients with heart failure. Clinicians should be aware that new onset of heart failure or exacerbation of pre-existing disease might occur in patients who begin TNF antagonist therapy. REFERENCES
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05056t1.jpg] |
| |||||||||

{kind=link}