 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
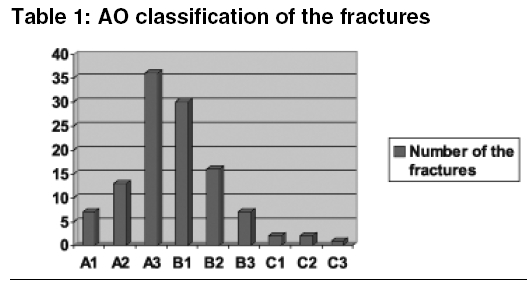
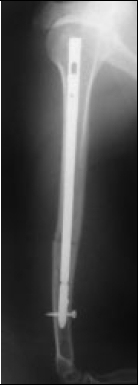
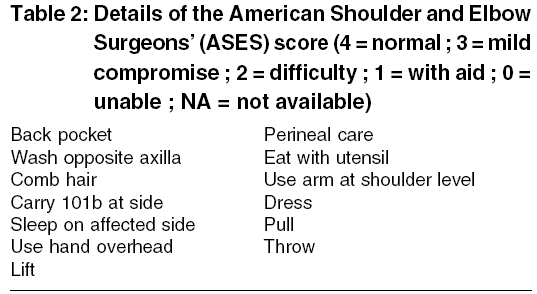
Indian Journal of Medical Sciences, Vol. 59, No. 10, October, 2005, pp. 436-442 Original Article Interlocking nailing of humeral shaft fractures a retrospective study of 114 patients Demirel M, Turhan E, Dereboy F, Ozturk A Departments and institutions, Ankara Bayindir Hospital Orthopaedics&Traumatology Code Number: ms05066 Abstract Background: Fractures of the humeral shaft are relatively common injuries. Literature suggests that humeral shaft fractures represent approximately 3 % of all fractures. There are several modalities for the management of diaphyseal humeral fractures. The latest investigations emphasize the concept of minimal exposure and rigid fixation. Keywords: Humerus fracture, Intramedullary nail, shoulder problems, plate fixation Introduction There are several modalities for the management of diaphyseal humeral fractures.[1],[2] Most acute humeral diaphyseal fractures can be treated adequately using non-operative methods. With improved implant design and surgical technique, operative treatment of humeral diaphyseal fractures increasingly has become accepted.[1] Indications for surgical treatment of humeral diaphyseal fractures are open fractures, segmental fractures, bilateral fractures, floating elbow injuries, fractures associated with vascular injuries or progressive neurological injury, and fractures in patients with multiple injuries.[1],[2] Such treatment offers several advantages. Although plate osteosynthesis can afford a rigid fixation and good functional recovery, its disadvantages have been reported like plate fixation does require a wide surgical exposure and more time when compared with intramedullary fixation.[1],[2],[3],[4] Locked intramedullary nails usually can be inserted using closed techniques, avoiding the extensive soft tissue dissection required for plating. Interlocking nails gives rotational stability, decrease the need for postoperative bracing and allowing early mobilization of the extremity.[3],[4] In this article we present our experience with locked antegrade nailing of acute humeral diaphyseal fractures in 114 patients. Materials and methods This is a retrospective review of 114 acute humeral diaphyseal fractures in 114 patients aged between 17- 88 years (average, 44.5 years), treated with antegrade AO unreamed humeral nail (AO-UHN, Synthes, Paoli, PA) for acute humeral fractures (n = 108) or for metastatic bone invasion at our hospital between January 1995 and December 2003 [Table - 1]. Information was obtained through review of clinic notes, photographs, therapy measurements and operative notes. All aspects of this study were approved by the Hospital′s Review Board. The exclusion criteria of this study were fractures involving adjacent joints, bone defect >3 cm, infection at the fracture site and patients younger than 17 years old. There were 79 male and 35 female patients. Mechanisms of injury included 85 motor vehicle accidents, two gunshot wounds, twelve pedestrian versus motor vehicle accidents, eleven falls from a height, four motorcycle accidents. Associated injuries occurred in 42 acute fractures: five head injury, eight chest injury, nine abdominal injuries, and twenty multiple fracture. Pathologic fractures were caused by metastasis from one breast cancer, two prostate cancers, one lung cancer, and two multiple myeloma. The average delay from trauma to operation was 12 hours (range, 2 hours-6 days; median, 18 hours). No bone grafting or bone cementing was performed in this study. There were twelve primary nerve palsies. For acute fractures, static locking was performed in 99 cases and dynamic locking in fifteen. Static locking was performed in all six pathologic fractures. Technique All open fractures are treated with immediate debridement and irrigation and exploration of the fracture site to ensure that the radial nerve is not entrapped. The entry portal for the nail is made using the anterolateral approach described by Riemer et al.[5] A 2-cm incision is made anterior to the midpoint of the acromion and the deltoid muscle is split longitudinally. A 1-cm incision is made in the rotator cuff in line with its fibers. An awl is used to create the entry postal just medial to the greater tuberosity in the sulcus between the greater tuberosity and the articular margin. The nails inserted without reaming. Canal diameter was measured on preoperative radiographs. The nail is inserted until its tip lies 1.5 to 2 cm proximal to the olecranon fossa. The proximal end of the nail is seated approximately 5 mm beneath the bone to prevent impingement. The nail should be inserted with the fracture well aligned to avoid intraoperative comminution. Proximal interlocking screw is placed with the use of a proximal drill guide. The screw should be directed so that it exits medially, distal to the articular margin of the humerus. A drill sleeve is inserted through a stab incision after soft tissues have been dissected bluntly down to bone. A hole is made with a 2.7-mm drill bit, and a 4-mm bicortical screw is inserted. Distal locking was performed using a freehand technique. Before the distal screw was inserted, the fracture site is compressed by placing an axial load on the elbow. Correct rotation is obtained by pointing the forearm and hand perpendicular to the ceiling. The patient′s arm was supported simply in a neck sling for the first few days after surgery. Range of motion (ROM) exercise was encouraged as early as tolerable. For acute fractures, the patients and radiographs were examined every 2 or 3 weeks until union was achieved. The operation time, time to union, shoulder functional score based on American Shoulder and Elbow Surgeons′score, the visual analogue pain score were recorded. The mean follow-up time was 41 months (range, 18-68 months). Statistical Analysis Mean values of operation time, time to union, shoulder functional score and visual analogue pain scores given with their own ranges. Results Two cases X-rays, managed with intramedullary nailing presented in [Figure - 1A-1B] and [Figure - 2A-2B]. One hundred-nine of the 114 (95.6%) fractures eventually united. The average time to union was 13 weeks (range, 10-36 weeks). Five fractures required autogenous bone grafting for delayed union or nonunion. Three of these five were either open fractures (Type II or Type IIIC) or closed fractures treated with an open technique. All fractures united after removal of the nail and fixation with DCP and bone grafting. To assess function, we used the American Shoulder and Elbow Surgeons′ (ASES) shoulder score for 13 activities of daily living requiring full shoulder and elbow movement [Table - 2]. The maximum possible score is 52 points. The average score was 48,5 (range, 40-52). We quantified pain using visual analogue scales, with zero being no pain and 10 extreme pain. The results range between zero and two with average 1,5. Complications included impingement due to proximal locking screws in two patients and prominent nail in three patients, transient postoperative radial nerve palsy in four patients. For fractures that were nailed in a closed manner, the operation time averaged 50 minutes (range, 38-122 minutes). For the twelve fractures treated with open nailing, the average operation time was 115 minutes. Discussion Isolated, low energy humeral shaft fractures usually can be treated satisfactorily with non-operative methods,[7],[8] but operative stabilization often is necessary for acute, high energy humeral shaft fractures to improve healing, fracture alignment, and functional results.[9],[10] In previous studies, the union rate of antegrade nailing of acute humeral fractures using nails with transfixing screws has ranged from 71% to 100%.[3],[11],[12],[13] However, the current authors also think that some lower union rates among reported clinical results might be accounted for by other factors, such as improper nailing direction, over-distraction of the fractures, or insufficient fixation stability, all of which could impair healing. When we look at the union rates, the reported recovery of shoulder function after antegrade nailing varies. In studies using Russell-Taylor nails, Ikpeme reported 22 (88%) patients with excellent or satisfactory recovery of shoulder function according to their Neer score.[12] Postoperative shoulder pain was caused mostly by proximal locking screws. Crates and Whittle reported 66 of 73 (90%) patients had full recovery of shoulder function.[3] Three patients had impingement: two caused by the proximal locking screw and one by a prominent nail. In contrast, Hems and Bhullar reported only 11 of 15 (73.3%) patients had excellent or satisfactory Neer scores.[11] They attributed these less than satisfactory results to intra-operative rotator cuff injury. However, their follow-up time (range, 1-42 months) was insufficient in terms of recovery of shoulder function. In the current study, with the exception of three (7.9%) patients with severe associated injury or bad general condition, patients with acute fractures had excellent or satisfactory recovery of shoulder joint function. The current authors think the following technical factors might be responsible for poor recovery of shoulder function: massive injury of the rotator cuff with inadequate repair, prominent nail head or locking screws, axillary nerve injury, and intra-operative comminution of the humeral head. More rigid locked intramedullary nails have better rotational control than flexible nails, which theoretically should decrease the frequency of nonunion. Riemer et al reported no nonunions in 28 acute humeral shaft fractures treated with Seidel nails.[5] Robinson et al, however, evaluated 30 humeral fractures treated with Seidel nails and found that 23% required additional treatment for delayed union.[15] Ingman and Waters reported union in 95% of 21 humeral fractures treated with modified Grosse-Kempf nails.[13] Ikpeme reported no nonunions in 30 acute humeral fractures treated with Russell-Taylor nails.[12] Lin et al, reported union in all 47 fractures treated with locked nailing.[2] Crates et al reported 94.5% union primarily with antegrade Russell-Taylor humeral nailing and two additional fractures united after bone grafting.[3] The most frequent criticism of antegrade humeral nailing has been its potentially deleterious effect on shoulder function. In a series of humeral fractures stabilized predominantly by Rush rods, Stern et al reported the development of adhesive capsulitis in 56% of fractures treated with antegrade nailing.[15],[16] The insertion point violated the rotator cuff in most of these patients, and nails frequently migrated proximally. Shoulder function returned to near normal after hardware removal. In 28 humeral fractures stabilized with antegrade Rush or Ender nails, Brumback et al reported excellent results in 18 (64%), good results in seven (25%), and poor results in three (11%).[9] Eight of the 10 shoulders with good or poor function had nails inserted through the rotator cuff. Seven of the eight had impingement symptoms develop that required hardware removal. Stern et al Brumback et al recommended an antegrade insertion point lateral and distal to the rotator cuff.[9],[16] Shoulder problems also have been reported with antegrade insertion of more rigid nails. Robinson et al reported that 12 of 30 (40%) humeral fractures treated with Seidel nails had protrusion of the nail above the humeral tuberosity, usually because of failure of the locking mechanism.[15] Five other patients in whom the nail was prominent also had poor shoulder function, which the authors attributed to local rotator cuff damage during insertion. Riemer et al also reported that five of 12 patients in whom a Seidel nail was inserted through a lateral deltoid incision had persistent shoulder stiffness.[5] No patients with nails inserted through an anterior deltoid incision had restricted shoulder motion; however, it sometimes took as many as 6 months for full shoulder function to return. In a series of 30 acute humeral fractures treated with antegrade Russell-Taylor nails, Ikpeme reported that six (20%) patients had shoulder pain and decreased shoulder abduction because of impingement of the proximal locking screws.[12] Removal of the proximal screws in five of these patients resulted in complete resolution of symptoms. Two other patients had proximal nail migration because of proximal interlocking through an area of comminution. In our series, shoulder pain because of nail impingement occurred in five (4.3%) patient in whom the nail was not properly countersunk. Shoulder pain was related to the proximal locking screws in two (1.7%) patients. Symptoms resolved in all patients after hardware removal. This retrospective review of 114 humeral shaft fractures treated with AO-UHN system revealed acceptable data′s in time to union, shoulder and elbow function, the operation time. Antegrade interlocking humeral nailing does not require extensive soft tissue dissection, infrequently requires bone grafting, does not require external immobilization, and may be more suitable for comminuted and segmental fracture patterns than plating or flexible nailing techniques. We believe that antegrade locked nailing in humeral shaft fractures are reliable and also effective in multiply injured patients. References
Copyright 2005 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms05066t2.jpg] [ms05066f1.jpg] [ms05066f4.jpg] [ms05066f3.jpg] [ms05066f2.jpg] [ms05066t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}